ABSTRACT
Background: The biothesiometer allows for a quick and accurate measurement of vibration thresholds, which, when combined with centile charts, provides an objective estimate of diabetic peripheral neuropathy progression. The goal of the current study was to assess diabetic patients’ early detection of peripheral neuropathy and associated consequences. Materials and Methods: Study was conducted on diabetes patients of medicine department of Maharishi Markandeshwar Super Speciality Hospital, MMIMSR, MM (DU), Mullana, after approval by the Institutional Ethics Committee (IEC). Patients were analysed for the vibration perception threshold (VPT) using Biothesiometer. After receiving their consent, socio-demographic parameters and previous medical history were noted on a case report form and patient’s QoL (Quality of Life) was analyzed using Diabetic Neuropathy (DN) 22 QoL questionnaire. The DN4 questionnaire was used to assess the presence of peripheral neuropathy pain. Results: In this research study total of 100 patients participated, of whom 55 were male patients and 45 were female patients The ages of these patients ranged from 26 to 86 years and mean of these patients was 55 years. The patients were divided into two distinct age groups: those under 50 and those above 50. Only 15 patients reported numbness, while the remaining 85 patients reported no abnormal sensations in their feet. However, when left foot and right foot readings were valuate on the biothesiometer, 9 patients had grade 1 say normal (15 volts), 12 patients had grade 2 (16-25 volts), and 79 patients had grade 3 (>25 volts). Conclusion: It was concluded that VPT was determined to be the gold standard or say best fit for detection of peripheral neuropathic pain in diabetes patients. Measuring VPT in diabetic patients with a biothesiometer may reduce the risk of developing neuropathic foot ulcers and foot amputations.
INTRODUCTION
A metabolic condition called diabetes mellitus (DM) is distinguished by unusually high blood sugar level. With the biggest number of diabetic patients, India is the second-largest region after China. Even in India’s rural populations, the number of people with diabetes has already been rising on a national level.1 Patients with DM have a 20-fold increased risk level of microvascular and macrovascular diseases than people with normal blood glucose levels.2 The most commonly and problematic consequence of DM is diabetic neuropathy. It also has a significant financial impact on diabetes patients care.3 Foot ulceration is a chronically and mostly observed complication in DM patients, with a prevalence of 6.3% globally,4 a recurrence level of 60%, and an elevated foot amputations risk.5
In India, nearly 80% of diabetic foot in DM patients are caused by peripheral neuropathy, trauma from walking barefoot or from wearing improperly fitting shoes, especially those living in rural. The consequences of diabetes complications like foot ulcer responsible for up to 50% of all hospitalizations for diabetes. According to estimates, 15% of diabetes patients have their lower limbs amputated, and between 10 and 15% of persons with diabetes may suffer foot ulcers in their life.6 Peripheral neuropathy in diabetes mellitus is a frequent and painful complication. Symptoms of peripheral neuropathy: Numbness, Tingling, Sharpnes, Burning pain. Approaches to identify peripheral diabetic neuropathy include loss of ankle jerk, reduced vibration threshold, monofilament testing, and biothesiometer.7
A biothesiometer is an instrument that can detect and quantify diabetic peripheral neuropathy in its early stages. It functions similarly to an electronic tuning fork. It carry a vibrating probe that detects neuropathy when connected to the bottom of the foot. The amplitude of vibrations is measured (volts) and can be adjusted by rotating the dial. Once the vibration has been detected, the individual being tested indicates. In young healthy people, the reading is low. It suggests they are vibration sensitive. As people get older, their biothesiometer readings rise, increasing their chances of developing ulcers. Amputations may be required because of delayed or non-healing ulcers, raising mortality.8 In the current study we assessed diabetic patients for early detection of peripheral neuropathic pain and consequences associated with it. We attempted to build a relationship between biothesiometer VPT readings and quality of life factors by which we detect how peripheral neuropathic pain effects the quality of life in diabetic patients. Also, the influence of factors like age of the patients, duration of the diabetes, smoking and alcoholic patients and how the peripheral neuropathy was maintained and determined for biothesiometer grades.
MATERIALS AND METHODS
An observational research study was carried on 100 patients for 6 months and the sample size was calculated using formula n= 4PQ / d2, where P, Q and d, are prevalence, 100- P and 20% of P respectively. The study protocol was approved by Institutional Ethics Committee (IEC) at Maharishi Markandeshwar Institute of Medical Sciences and Research (MMIMSR), Mullana having ethical clearance number: 2126. The study includes inpatients over the age of 18 years who are taking antidiabetic therapy and those patients who are willing to participate in this study. The patients of other causes of neuropathy such as vasculitis, amyloidosis, toxic neuropathy, AIDS, renal failure, symptomatic lumbosacral spine disease, Infected foot ulcers and those who were refused to participate in the research study were excluded from the study. The study was conducted on digital biothesiometer vibrometer machines Figure 1(KODYS- Destination of Diabetic foot care VPT-774 and model no: KD36 TB74 64KR).
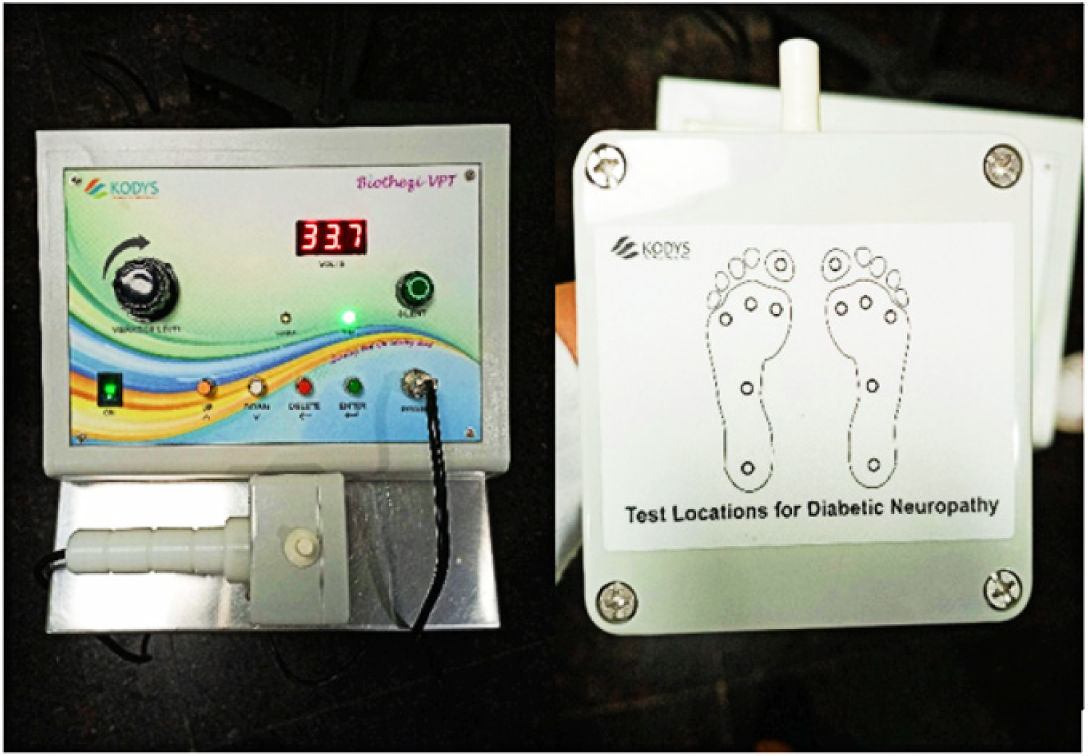
Figure 1.
Biothesiometer Vibrometer Machine.
The vibrometer has a 0-50 volt vibration output range. The biothesiometer measures the threshold of vibration appreciation. The stimulus’s amplitude measured (volts) is steadily increased when the vibratory sensation threshold value is reached and the stimulus is received by the patient. Patients having a threshold of >25 volts (grade 3) are more likely to develop ulcers in the future. The biothesiometer has a sensitivity of 80% and specificity of 99% for detecting neuropathy.8
Right and left feet’s neuropathy spots were digitally recorded using a connected laptop (Figure 2). There were six areas on each foot’s plantar aspect that were pointed: the plantar aspect of the big toe, three metatarsal heads, the instep, and the heel. The parameters were measured in volts.

Figure 2.
Handling of Biothesiometer Vibrometer Machine.
The DN4 (Douleur Neuropathique 4) is one of the questionnaires that can be used to diagnose neuropathic pain. The DN 4 questionnaire is a ten-item clinician-administered questionnaire. It includes aspects of how the patient perceives pain, as well as whether the sensation has reduced (hypoesthesia) to touch or pinprick, and whether mild brushing enhances or produces discomfort for the patient (allodynia). The questionnaire was written in French at first, but the same team quickly translated it into English. Because of its simplicity, the scale has been widely used since 2005. It is utilised for diagnosis, allowing the clinician to evaluate whether the pain is neuropathic.9
DN 22 QoL (Diabetic Neuropathy Quality of Life Questionnaire) designed to measure the effects of diabetic neuropathy on quality of life. DN 22 QoL composed of 4 parts- Physical health, Emotional / Psychological health, Social health, General health. DN 22 QoL consists of 22 items and used to scoring QoL.
RESULTS
100 participants were enrolled in the trial, of whom 55 were men and 45 were women. Ages of the patients ranged from 26 to 86, with a mean age of 55. There were 67 patients over the age of 50 years and 33 patients under 50 years.
Only 15 patients reported numbness in their feet, while the remaining 85 patients reported no abnormal sensations in their feet. The mean score on the biothesiometer for the right feet and left feet was 34.6 and 35.0 volts with the lowest value for both feet was 12.9 and the highest value was 49.8 volts as shown in Table 1.
| Statistics | Right foot VPT (average) | Left foot VPT (average) |
|---|---|---|
| Mean | 34.6 | 35.0 |
| Mode | 46.1 | 34.1 |
| Std Deviation | 10.7 | 10.6 |
| Minimum | 13.3 | 12.9 |
| Maximum | 49.8 | 49.4 |
Neuropathy was defined and categorized on the basis of grades. 9 patients who responded to a stimulus value of <15 volts were considered to be grade 1 neuropathy. 12 patients could appreciate the stimulus of 16-25 volts and were identified as having grade 2 neuropathy in this group. The patients whose threshold value was > 25 volts had grade 3 neuropathy. This group included 79 patients (Table 2).
| Neuropathy Grades | Frequency (no of patients) |
|---|---|
| Grade 1 | 9 |
| Grade 2 | 12 |
| Grade 3 | 79 |
The age distribution revealed that grade-1 and grade -2 neuropathy was more prevalent in patients <50 years of age than in those who were older than 50 years. But grade-3 neuropathy was frequently seen in patients > 50. Out of 100 patients, 35 patients were smoker, 33 were alcoholic, 26 were addict to both whereas, 06 were neither smoker nor alcoholic. For measuring their VPT, results showed that smoker and alcoholic patients had more risk of neuropathic pain as compared to non- Smoker and non- alcoholic as shown in Table 3.
| Grades | Smoker | Alcoholic | Both (Alcoholic+Smoker) | None | <50 | > 50 |
|---|---|---|---|---|---|---|
| Grade 1 | 1 | 2 | 3 | 3 | 7 | 2 |
| Grade 2 | 7 | 4 | 1 | 0 | 7 | 5 |
| Grade 3 | 27 | 27 | 22 | 3 | 19 | 60 |
| Total | 35 | 33 | 26 | 6 | 33 | 67 |
| % of Grade 3 | 77 | 82 | 85 | 50 | 58 | 90 |
Neuropathic pain was determined in 100 patients by using DN 4 Questionnaire. Patients with DN4 score >4 were 20 patients and with DN<4 score were 80 patients. Patients with DN4 score >4 had a higher mean VPT score than those with DN4 score <4. In Table 4, correlation of DN 4 score and biothesiometer shown. 9 patients had grade-1 neuropathic pain scored DN<4 value. 12 patients had grade-2 neuropathic pain, in which 11 patients scored DN<4 and 1 patient had DN>4 score. 79 patients were suffering from grade-3, in which 60 scored DN<4 value and 19 scored DN>4.
| Grade | DN <4 | DN >4 | Total |
|---|---|---|---|
| Grade 1 | 9 | 0 | 9 |
| Grade 2 | 11 | 1 | 12 |
| Grade 3 | 60 | 19 | 79 |
100 patients with DN were concluded for DN 22 QoL Questionnaire to detect the effects of neuropathic pain on quality of life on the basis of QoL score as shown in Table 5. Patients with poor QoL score was higher in peripheral pain and scored higher VPT value. 13 patients scored good QoL (<10), 15 patients scored above avg QoL (11-30), 25 patients scored avg QoL score (31-45), 22 patients scored below avg QoL (46-55) and 25 patients had poor QoL (above 55).
| Quality of life | Grade 1 | Grade 2 | Grade 3 | Total |
|---|---|---|---|---|
| Good QoL (<10) | 6 | 2 | 5 | 13 |
| Above Avg QoL (11-30) | 3 | 4 | 8 | 15 |
| Avg. QoL (31-45) | 0 | 6 | 19 | 25 |
| Below Avg QoL (46-55) | 0 | 0 | 22 | 22 |
| Poor QoL (above 55) | 0 | 0 | 25 | 25 |
DISCUSSION
This study for the first time attempted to build a relation between the biothesiometer readings with DN 4 neuropathique score and QoL score and then on the basis of score detects severity of the peripheral neuropathy in diabetic patients.
According to studies by Basit et al. the incidence of diabetes is between 5-7%; given that the incidence of foot ulcers is 10%, we may have approximately one million (recalculated for a population of 20 crore) diabetic foot ulcer sufferers.10 Furthermore, amputation mortality is estimated to reach 30% after one year, 50% after three years, and 70% after five years.11 Diabetes mellitus has become a global epidemic in the world. Amputations of the lower extremities due to diabetic foot after long-term diabetic neuropathy afflict 30% of type 2 diabetics. The yearly population-based incidence of foot ulceration ranges from 1.0 to 4.1 percent, and the prevalence among diabetics ranges from 4 to 10%, signifying that the lifelong risk may be as high as 25%.12
According to Young MJ et al. study the patients with baseline threshold elevated above a fixed value (i.e., 25 volts with the biosthesiometer) were seven times more likely to develop foot ulcers.8 In this study, biothesiometer was considered as the Gold Standard test for the early detection of peripheral neuropathy in diabetes mellitus patient. Patients that suggested no any symptoms of neuropathy pain (85 patients), however when they were evaluated with a biothesiometer, 91 patients (including all 15 who had a history of numbness) had sensory neuropathy of grade 2 or 3. Our patient sample size was small, but it was a study to see if patients had neuropathy and to educate them on proper foot care.
According to Boulton et al., VPT provides a strong indication of “risk” for future ulceration across a wide range of ages and durations of diabetes.13 The severity of neuropathy did not appear to be affected by gender, 40 male patients had grade-3 and 39 female patients had neuropathy grade-3, however age and duration of the diabetes showed as association with peripheral neuropathy. 60 patients who were >50 years of age had grade -3 neuropathy and <50 years age 19 patients that scored grade -3 neuropathy.
Smoker and alcoholic patients had more risk of peripheral neuropathy, scored neuropathy grade -3 other than non-smoker and non- alcoholic patients. The possibility of the neuropathic pain increases as the older age, duration of diabetes, smoking, alcohol consumption and their biothesiometer readings rise, increasing their chances of developing ulcers. Amputations may be required as a result of delayed or non- healing ulcers, raising mortality. Jayaprakash et al. assessed the role of several bedside methods in the evaluation of peripheral neuropathy in a patient sample of 1044 and found that different beside methods of neuropathy evaluation had varying sensitivity and specificity.14
As a result, we can recommend that diabetic patients to undergo biothesiometry at regular intervals as part of a routine diabetic check-up, which can facilitate in the early detection of peripheral neuropathy and future therapy to prevent disease progression that leads to diabetic ulcers.
CONCLUSION
VPT is considered as the gold standard for diabetic peripheral neuropathy diagnosis. In our country, there is a scarcity of data on measuring VPT in diabetics with a biothesiometer. The biothesiometer is an important tool for detecting and grading peripheral neuropathy. Other bedside approaches are straightforward and practical, but their results may be biased by subjective differences. As a result, the biothesiometer may be used to predict the development of neuropathic foot ulcers in the future, thereby chances of foot amputations may be reduced.
References
- Pradeepa R, Mohan V. Prevalence of type 2 diabetes and its complications in India and economic costs to the nation. Eur J Clin Nutr. 2017;71(7):816-24. [PubMed] | [CrossRef] | [Google Scholar]
- Gregg EW, Sattar N, Ali MK. The changing face of diabetes complications. Lancet Diabetes Endocrinol. 2016;4(6):537-47. [PubMed] | [CrossRef] | [Google Scholar]
- Vinik AL. Epidemiology of the complications of diabetes. Clin Sci Pract. ;1995:221-87. [PubMed] | [CrossRef] | [Google Scholar]
- Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y, et al. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann Med. 2017;49(2):106-16. [PubMed] | [CrossRef] | [Google Scholar]
- Ahmad J. The diabetic foot. Diabetes Metab Syndr. 2016;10(1):48-60. [PubMed] | [CrossRef] | [Google Scholar]
- Rajaei E, Jalali MT, Shahrabi S, Asnafi AA, Pezeshki SMS. HLAs in autoimmune diseases: Dependable diagnostic biomarkers?. Curr Rheumatol Rev. 2019;15(4):269-76. [PubMed] | [CrossRef] | [Google Scholar]
- Kodl CT, Seaquist ER. Cognitive dysfunction and diabetes mellitus. Endocr Rev. 2008;29(4):494-511. [PubMed] | [CrossRef] | [Google Scholar]
- Young MJ, Breddy JL, Veves A, Boulton AJ. The prediction of diabetic neuropathic foot ulceration using vibration perception thresholds. A prospective study. Diabetes Care. 1994;17(6):557-60. [PubMed] | [CrossRef] | [Google Scholar]
- Madani SP, Fateh HR, Forogh B, Fereshtehnejad SM, Ahadi T. Validity and reliability of the Persian (Farsi) version of the DN4 (Douleur Neuropathique 4 Questions) questionnaire for differential diagnosis of neuropathic from non-neuropathic pains (Farsi). Pain Pract. 2014;14(5):427-36. [PubMed] | [CrossRef] | [Google Scholar]
- Basit A. Economic burden of diabetic foot at a tertiary care hospital of Karachi, Pakistan. Proceedings. Pulse Int, Reg conference at FJMC Lahore. 2006;7:6 [PubMed] | [CrossRef] | [Google Scholar]
- Jawaid SA. Management of diabetic foot ulcers; some bitter facts and harsh realities. Pak J Med Sci. 2006;22(2):97-100. [PubMed] | [CrossRef] | [Google Scholar]
