ABSTRACT
Background: Thyroid disorder is becoming increasingly common in India. Thyroid disorder affects around forty million people in India. The number of cases in Telangana is increasing at an alarming rate. This survey aims to investigate the causes of an increase in thyroidism cases and to present data for debate at a thyroid problems symposium. Materials and Methods: The current online survey has been conducted by posing 22 questions regarding the type of thyroid disorders and the predisposing factors responsible for it by distributing online Google forms randomly to a large group of the Telangana population which includes 2000 individuals. Results: The results obtained from the survey indicated that the most common thyroid disorder prevailing in Telangana is Hypothyroidism. Females are affected most with hypothyroidism to an extent of 62.3%. The cases of Hypothyroidism in pregnancy were found to be less (27.4%) in comparison to non-pregnant females (72.6%). Vegetables and fruits were found to be included very less in their respective diets (16.9%). Majority of the Hypothyroid patients have shown disinterest (68.4%) in performing exercises during Hypothyroid episodes. In many female hypothyroid participants, there are menstrual irregularities. TSH estimation remains the most popular test among the thyroid patients. Conclusion: The outcome of the current survey suggests that there is a need to maintain a healthy diet which includes fruits and vegetables and regular exercises to maintain a healthy BMI. Females are advised to focus on the menstrual irregularities due to Hypothyroidism. If the above suggested measures were taken, then the hypothyroidism can be effectively controlled in Telangana where the incidences are alarmingly high.
INTRODUCTION
The thyroid is a 2-inch-long butterfly shaped organ weighing short of what one ounce. Situated before the neck underneath voice box it has two lobes, one on each side of windpipe.1 The thyroid is the one of the organs that makes up endocrine framework, the organs of the endocrine glands produce and store chemicals into and discharge them into circulatory system, the chemicals then, at that point, travel all through the body and direct the activity of the body cells.2,3 The thyroid organ makes two thyroid hormones, Triiodothyronine (T3) and Thyroxine (T4). T3 is produced using T4 and is more dynamic hormone that directly influence the tissues.4 Thyroid hormones influence digestion, mental health, breathing heart and nerves, internal heat level muscle strength, skin dryness, menstrual cycle weight and cholesterol level.5 Thyroid hormone production is controlled by the thyroid stimulating hormone, which is otherwise called TSH, which is made by the pituitary organ in the brain.6,7 At the point when thyroid hormone levels in the blood are low the pituitary releases the TSH.8,9 When thyroid hormone levels are high the pituitary responds by the dropping TSH generation. Hyperthyroidism alludes to the common morbid state of thyroid hormone lack.10 It happens when the thyroid gland doesn’t make sufficient thyroid hormones to meet the body needs. Thyroid hormones regulates digestion the manner in which the body uses and impacts virtually every organ in the body.11,12 Without sufficient thyroid hormones a considerable amount of the body functions delayed down in some cases.13 It can prompt extreme unfavorable wellbeing impacts and eventually death in light of the huge variation in the clinical presentation and general shortfall of side effect explicitness.14,15 The meaning of the hypothyroidism is prevalently biochemical for sure or clinical. Primary hypothyroidism is characterized as a thyroid stimulating hormone TSH concentration above the reference range and free thyroxine concentration beneath the reference range.16 Mild or subclinical hypothyroidism which is regularly viewed as an indication of early thyroid failure is characterized as the concentration above the reference range and free thyroxine concentration with normal range.17,18 Primarily females are generally impacted with the condition of hypothyroidism of extent 62.3% in Telangana.19 Though pregnant women were less impacted compared with the normal females of around 27.4% in Telangana. Hypothyroidism is more normal in patients with immune system sickness, for example, type one diabetes, autoimmune gastric atrophy and such type of illnesses it can likewise happen part of numerous immune system endocrinopathies.20,21 Therefore the current online survey was designed with a questionnaire to gather information about the status of thyroid disorders in a set of urban Telangana population and to understand the cause behind this high rate of thyroid disorders.
MATERIALS AND METHODS
Google form was utilized to disseminate the questionnaire (2000 participants). Most of the participants (1858) has responded positively to the survey. The questionnaire included 22 questions. The questionnaire discusses about number of family members suffering from thyroid diseases, what type of thyroid diseases are predominantly seen, how many thyroid cases during pregnancy, diet during thyroid disease, how many thyroid sufferers perform, any preexisting disease with thyroid issues, any irregularities in menstrual cycle, any PCOD or PCOS problems with thyroid and ancestors in the family having thyroid disorders. The data of the participants were collected and further tabulated and analyzed.
Factors that lead to the design of the survey
A recent article published in Times of India on February, 2022, titled as “thyroid disorders on the rise among women” stated that Telangana stands fourth in India in relation to endocrine disorders triggered largely due to high consumption of junk street food as per the experts. According to the Union health and family welfare ministry’s latest data, Telangana has 5763 women caseloads (per lakh population) with only Kerala, Jammu and Kashmir and Delhi ranked higher. Despite the thyroid disorder has genetical input mostly among woman, but currently it has been witnessed that thyroid issues occurred in females in whom it does not run in families. Consumption of junk food cooked in adulterated oil causes goitre and is one of the predisposing factors for rise in thyroid cases as articulated by Dr. Sudhakar, President of Telangana Endocrine Society. According to the researchers, a study is urgently required because the state has a high prevalence of obesity and diabetes.22 Thyroid disorder can lead to problems such as high blood pressure and high cholesterol and the state already has high incidences of heart problems.23 Endocrinologists revealed that four southern states except Karnataka are among the top 10 states with large number of thyroid disorder cases which indicates how food habits play a role.24 Dr. K.D Modi, Secretary of the Telangana Endocrinologists Society, said that the higher prevalence for thyroid disorders is due to the accessible, simple and inexpensive thyroid tests now a day’s. In past the thyroid test would take 2 days of time as the sample has to be sent to Mumbai. By considering the exponential rise in thyroid cases every year and also the unbalanced diet that is followed by most of the Telangana people, we designed an online survey through distribution of Google forms which comprises of questionnaire about the lifestyle and food habits of Telangana people in Thyroid diseases as well as in non-thyroid cases and the treatment they follow during hypothyroidism and hyperthyroidism etc.
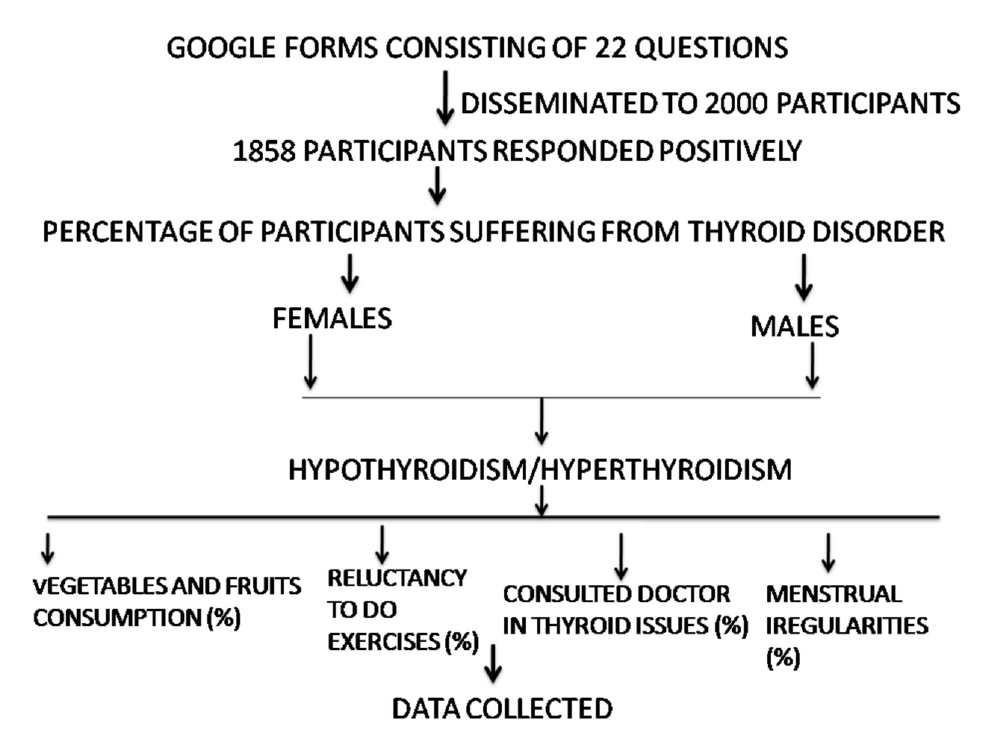
Flow Chart 1.
Consort chart of the survey.
RESULTS
The following questions have been posed in the questionnaire and the responses of the participants are as follows: Females are suffering more from thyroid disorders (60%) in Telangana with Hypothyroidism (54.3%) being the most commonly seen problem. A Major group of population suffering from thyroid issues in Telangana is seen to follow unbalanced diet (48.8%) which lack’s vegetables, fruits and nutrients. A majority of the thyroid patients (68.4%) mentioned that they are not interested in performing regular exercises which is a disturbing fact. A large group of population (78.5%) said no to the ancestral history of thyroid diseases. In a definite set of female population (41.3%) menstrual irregularities found during thyroid disorders. Weight gain is the major symptom found in hypothyroid females of Telangana (28.7%). Thyroidism associated with goiter is 33.8%. Most of the thyroid patients in Telangana have consulted a doctor (68.8%) and the doctor referred for TSH estimation (66.3%). A large group of patients are still not avoiding goitrogenic foods such as cabbage, cauliflower, soya etc. (47.4%). Survey reveals that the prognosis of the thyroid treatment that includes reduction in TSH levels back to normal in Hypothroidism is only to an extent of 32.5% and in Hyperthyroidism the TSH levels raised back to normal in only 16.3% patients indicating that the thyroid issues are not adequately controlled in Telangana. The results are depicted in Table 1 and Figure 1.
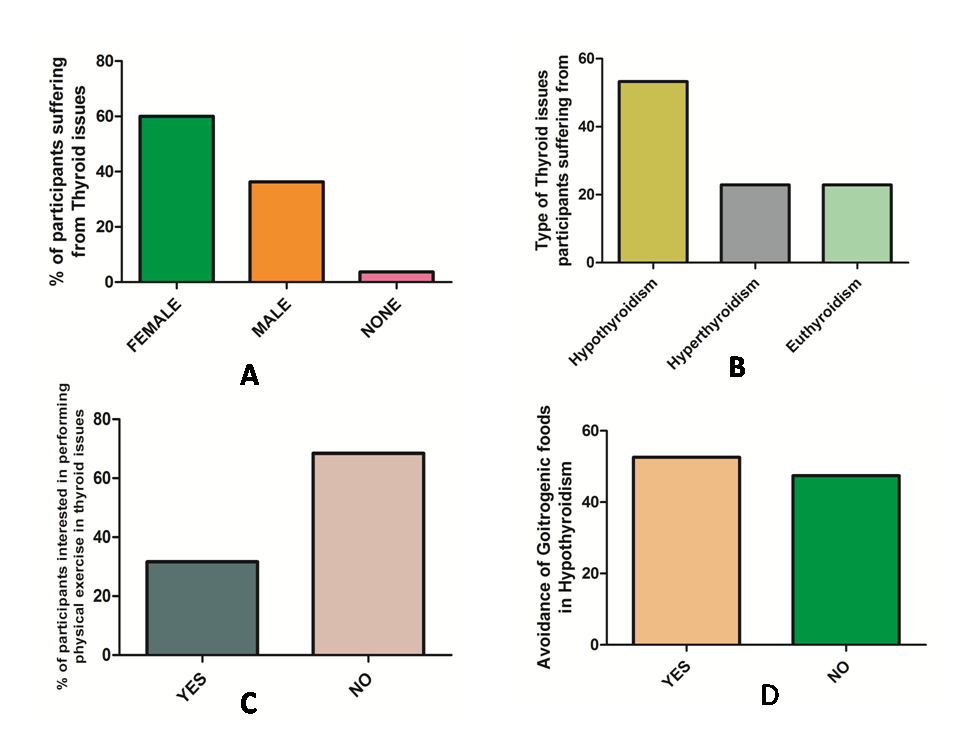
Figure 1.
Responses of the Participants in Thyroid survey. A. Percentage of participants suffering from thyroid disorders. B. Type of thyroid issues participants are suffering from. C. Percentage of participants interested in physical exercises during thyroid problems. D. Percentage of participants avoided goitrogens during Hypothyroidism.
| Q.No | Question | Response of the participants |
|---|---|---|
| 1 | Do you/any of your family members affected with Thyroid disease? | Yes= 57.5%, No= 42.5%. |
| 2 | If yes then who is affected? | Female= 60%. Male=36.3%, None=3.7%. |
| 3 | Which type of thyroid disease is affected to you/your family member? | Hypothyroidism=52.3%, Hyperthyroidism=22.9%, None=22.9%. |
| 4 | Do any of your family member affected with thyroid during pregnancy or after pregnancy? | Yes=26.3%, No=73.7%. |
| 5 | What type of diet you/they prefer to control their thyroid? | Eggs and all types of meat=23.8%, Veggies and fruits=16.3%, Diary products and iron supplements=11.3%, None of the above=48.8%. |
| 6 | Will you perform any regular exercises to control thyroid levels? | Yes=31.6%? No=68.4%. |
| 7 | Do you/they suffer from any other coexisting disease with thyroid issues? | Yes=15.2%, No=84.8%. |
| 8 | Is the thyroid disease before seen in your ancestors? | Yes=21.5%, No=78.5%. |
| 9 | Have you seen any irregularities in your menstrual cycle? | Yes=41.3%, No=58.8%. |
| 10 | Do you have any PCOD/PCOS problems? | Yes=17.5%, No=82.5%. |
| 11 | What are the effects seen in a thyroid patient? | Weight gain=28.7%, Lack of stamina=10%, Fatigue=11.2%, All the above=50%. |
| 12 | Do you have a large swelling in the neck (Goiter)? | Yes=33.8%, No=66.2%. |
| 13 | Did you have any unexplained weight loss or weight gain? | Yes=58.8%, No=41.3%. |
| 14 | Did you have any changes in the appetite? | Yes=48.8%, No=51.2%. |
| 15 | Do you often feel? | Hot=25.3%, Cold=17.7%? Normal=57%. |
| 16 | Have you consulted doctor? | Yes=68.8%, No=31.3%. |
| 17 | If consulted, what type of test referred by the doctor? | TSH=66.3%, T3=5%, T4=16.3? None=12.5%. |
| 18 | Have you avoided cabbage, cauliflower and soya? | Yes=52.6%, No=47.4%. |
| 19 | Are you taking Thyroid medicines with Coffee or Tea? | Yes=26.3%, No=73.8%. |
| 20 | What is the outcome of the thyroid treatment? Thyroid hormone levels after treatment? | Decreased=32.8%, Increased =16.3%, Neutral=22.5%, No change=28.7%. |
| 21 | Have you given blood sample for analysis of TSH/T3/T4 levels with fasting or after having food? | With fasting=67.5%, With food=30%, None of these=2.5%. |
| 22 | Time of consumption of thyroxine tablets? | 5 AM-10 AM=70%, 10 AM-12 AM=16.2%, 12 PM-6 PM= 3.8%, 6 PM-9 PM= 10%. |
DISCUSSION
Thyroid diseases are among the most common endocrine disorders worldwide. These disorders are frequently misdiagnosed. In general, a lack of awareness and comprehension of the impact of thyroid disorders can lead to people going undiagnosed. Thyroid function is crucial to human health, so any disruption to that function can have serious consequences. Bone density loss, slow growth, congestive heart failure, arrhythmia, constipation, weight gain, and myxedema have all been linked to hypothyroidism. Patients with hyperthyroidism, on the other hand, may exhibit sensitivity to stress, decreased body mass, increased perspiration, diarrhoea, trembling, hypocholesterolemia, heat intolerance, or irregular menstrual cycles. The purpose of this online study is to determine the general population’s degree of knowledge of thyroid disease signs, risk factors, and preventive actions.25 The outcome of the current research indicates that hypothyroidism is the most prevalent kind of thyroid disease in Telangana. This elevated prevalence of hypothyroidism is due to lifestyle factors such poor dietary habits, insufficient exercise, and the use of goitrogenic foods. More than 60% of respondents, however, indicated that they had sought medical attention at the onset of hypothyroidism symptoms, implying that they had a awareness of the issue. The vast majority of people (78.5%) rejected a family history of thyroid disorders. Thyroid issues are a common cause of menstruation abnormalities in women (41.3%). Women with hypothyroidism in Telangana, India, tend to put on weight more frequently than men (28.7%). Goiter is related with thyroid disease in 33.8% of cases. Thyroid patients in Telangana are fairly likely to seek medical attention (68.8%) and have their physicians refer for TSH estimation (66.3%). Goitrogenic foods, including cabbage, cauliflower, soy, etc., are still consumed by a sizable percentage of patients (47.4%). Thyroid problems are not adequately handled in Telangana, Telangana, according to the current survey. The prognosis of thyroid treatment, as measured by a return to normal TSH levels, is only 32.5% in Hypothroidism and 16.3% in Hyperthyroidism. Studies of this kind on hypothyroidism can be very useful in guiding doctors’ attention during first consultations and subsequent check-ins with patients.
CONCLUSION
The findings of this online survey on 2000 participants has triggered some alarming facts which needs to be addressed immediately. Thyroid cases are at its highest (53%) in Telangana. Unbalanced diet, lack of regular exercises, menstrual irregularities during thyroid disorders, weight gain in Hypothyroidism, increased consumption of goitrogenic foods during thyroid issues are the major issues that has been identified during our survey. These issues are required to be corrected at an earliest to avoid the sharp rise in thyroid disorders in Telangana.
Cite this article
Kadiri SK, Kumar RR, Jyothi K, Ramya K, Annam LD. A Survey on Thyroid Disorders and its Predisposing Factors in the Telangana Population. J Young Pharm. 2023;15(2):368-71.
ACKNOWLEDGEMENT
The authors are grateful to the management of Marri Laxman Reddy Institute of Pharmacy, Hyderabad for supporting our research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
References
- Klein I, Danzi S. Thyroid disease and the heart. Circulation. 2007;116(15):1725-35. [Google Scholar]
- Tunbridge WM, Evered DC, Hall R, Appleton D, Brewis M, Clark F, et al. The spectrum of thyroid disease in a community: The Whickham survey. Clinical Endocrinology. 1977;7(6):481-93. [Google Scholar]
- Duntas LH. Thyroid disease and lipids. Thyroid. 2002;12(4):287-93. [Google Scholar]
- Cooper DS, Biondi B. Subclinical thyroid disease. The Lancet. 2012;379(9821):1142-54. [Google Scholar]
- Casey BM, Leveno KJ. Thyroid disease in pregnancy. Obstetrics and Gynecology. 2006;108(5):1283-92. [Google Scholar]
- Negro R, Mestman JH. Thyroid disease in pregnancy. Best Practice and Research Clinical Endocrinology and Metabolism. 2011;25(6):927-43. [Google Scholar]
- Weetman AP. Autoimmune thyroid disease. Autoimmunity. 2004;37(4):337-40. [Google Scholar]
- Danzi S, Klein I. Thyroid disease and the cardiovascular system. Endocrinology and Metabolism Clinics. 2014;43(2):517-28. [Google Scholar]
- Weetman AP. Autoimmune thyroid disease: Propagation and progression. European Journal of Endocrinology. 2003;148(1):1-9. [Google Scholar]
- Levy EC. Thyroid disease in the elderly. Medical Clinics of North America. 1991;75(1):151-67. [Google Scholar]
- Uygur MM, Yoldemir T, Yavuz DG. Thyroid disease in the perimenopause and Postmenopause period. Climacteric. 2018;21(6):542-8. [Google Scholar]
- Brent GA. Environmental exposures and autoimmune thyroid disease. Thyroid. 2010;20(7):755-61. [Google Scholar]
- Mouradian M, Abourizk N. Diabetes mellitus and thyroid disease. Diabetes Care. 1983;6(5):512-20. [Google Scholar]
- Jones DD, May KE, Geraci SA. Subclinical thyroid disease. The American Journal of Medicine. 2010;123(6):502-4. [Google Scholar]
- Mitrou P, Raptis SA, Dimitriadis G. Thyroid disease in older people. Maturitas. 2011;70(1):5-9. [Google Scholar]
- Mandel SJ, Brent GA, Larsen PR. Levothyroxine therapy in patients with thyroid disease. Annals of Internal Medicine. 1993;119(6):492-502. [Google Scholar]
- Mokshagundam S, Barzel US. Thyroid disease in the elderly. Journal of the American Geriatrics Society. 1993;41(12):1361-9. [Google Scholar]
- Rashid M, Rashid MH. Obstetric management of thyroid disease. Obstetrical and gynecological survey. 2007;62(10):680-8. [Google Scholar]
- Kim YA, Park YJ. Prevalence and risk factors of subclinical thyroid disease. Endocrinology and Metabolism. 2014;29(1):20-9. [Google Scholar]
- Mulder JE. Thyroid disease in women. Medical Clinics of North America. 1998;82(1):103-25. [Google Scholar]
- Feldman AZ, Shrestha RT, Hennessey JV. Neuropsychiatric manifestations of thyroid disease. Endocrinology and Metabolism Clinics. 2013;42(3):453-76. [Google Scholar]
- Jara LJ, Navarro C, Brito-Zerón MD, García-Carrasco M, Escárcega RO, Ramos-Casals M, et al. Thyroid disease in Sjögren’s syndrome. Clinical Rheumatology. 2007;26(10):1601-6. [Google Scholar]
- Mehran L, Amouzegar A, Azizi F. Thyroid disease and the metabolic syndrome. Current Opinion in Endocrinology, Diabetes and Obesity. 2019;26(5):256-65. [Google Scholar]
- Luo Y, Kawashima A, Ishido Y, Yoshihara A, Oda K. Iodine excess as an environmental risk factor for autoimmune thyroid disease. International Journal of Molecular Sciences. 2014;15(7):12895-912. [Google Scholar]
- Alyahya A, AlNaim A, AlBahr AW, Almansour F, Elshebiny A. Knowledge of Thyroid Disease Manifestations and Risk Factors among Residents of the Eastern Province, Saudi Arabia. Cureus. 2021;13(1) [Google Scholar]