ABSTRACT
Background
Asthma is a rapidly increasing chronic respiratory disease worldwide. Inhalation drug therapy plays a vital role in asthma management because of immediate pharmacological response. Currently, a wide range of inhaler devices are being used worldwide, among which Metered Dose Inhalers (MDIs) are most commonly prescribed. Adherence with therapy directly depends upon the patient’s satisfaction with inhalation therapy. The current study aimed to determine the asthma patient’s satisfaction with inhalers. As well as the influence of pharmacist led educational intervention upon inhaler satisfaction of asthma patients.
Materials and Methods
The present cross-sectional study recruited 207 physician diagnosed adult asthmatics who were currently using MDI. The patient’s satisfaction with their inhaler was accessed through the study tool- FSI-10 questionnaire. After baseline observations, pharmacist led educational intervention was delivered to asthma patients. The pharmacist personally educated study subjects regarding the proper usage technique and importance of MDIs. Moreover, literature pamphlets containing inhaler technique were provided to patients at the end of intervention. Pre and post intervention satisfaction with inhaler was determined statistically.
Results
Majority of the asthma patients (197) i.e., 95.2% were observed to have low satisfaction regarding their pressurized meter dose inhalers. Only 4.8% patients presented high satisfaction with inhaler at baseline. However, patients’ satisfaction with their inhalers was raised from 4.8% to 58.5% as the result of intervention. The univariate analysis of the FSI-10 questionnaire data demonstrates a noteworthy association of the intervention given to patients regarding inhaler usage with its effect on the patients’ level of satisfaction with the inhaler. The current study showed p-value of 0.001 (p <0.05) which statistically proves that there is a significant effect of intervention on patients’ level of satisfaction with inhalers.
Conclusion
During baseline survey, majority of the patients presented poor satisfaction with their inhaler. But post intervention evaluation presented an enhancement in patient’s satisfaction with inhalers. Concluding that pharmacist led educational intervention proved to be effective in improving the patient’s satisfaction with inhalers.
INTRODUCTION
Respiratory diseases execute millions and cause enduring to millions more. Dangers to our lung well-being are all over, and they begin at an early age, when we are generally with low immunity. Luckily, a large number of these risk are avoidable and their results treatable. By acting now, we can spare lives and avoid enduring around the world.1 Asthma is the most prevalent chronic disease among existing respiratory diseases. Asthma is defined by “Global Initiative for Asthma” (GINA) guidelines as: “A heterogeneous disease that is commonly characterized by reversible chronic inflammation of bronchioles and airways. It is classified by the history of symptoms such as wheezing, Shortness of Breath (SOB), chest tightness and chronic cough that differs in intensity over extent and time and with variable expiratory airflow limitation”.2 Status asthmaticus is viewed as the greatest component of the grimness and mortality on the planet. These asthma intensifications make a tremendous weight on the personal satisfaction of the patients and their families. Regardless of its enlarged overall event, the example of asthma hospitalizations differs between various nations.3
Around 300 million individuals globally are right now experiencing asthma, with evaluations proposing that by consistently the predominance of asthma increments worldwide would raise by half.4 In Pakistan, approximately 6 million people are suffering from asthma. Pakistan’s largest city according to population; Karachi comprises about 8-10% chronic asthma suffering population; every 250th death in this large city is due to severe asthma exacerbations.5
Although this disease can never be cured completely, appropriate treatment along with prevention and management can control the disease substantially and allow people with asthma to gain improved quality of life.6 Rapid acting bronchodilator medications are used to relieve acute symptoms of asthma.7 People with persistent symptoms are required to administer long-term medications on regular basis to control the inflammation and prevent asthma symptoms and severe exacerbations.3 Medications are only used to alleviate the exacerbated symptoms and prevent future asthma attacks; management of asthma on the whole includes the avoidance of asthma triggers along with medical treatment.8
“National Asthma Education and Preventive Program” (NAEPP) and “World Health Organization” (WHO) provides following guidelines for diagnosis and management of asthma: Evaluating asthma severity then managing asthma control, Provision of patient education to promote patient care, Control of environmental trigger factors and comorbid conditions that effect asthma, Utility of pharmacological active agents in treatment for asthma.9
Since, the appropriate management of asthma mostly depends on adherence to medication. And the most important medication is being considered the inhalation drug therapy. The usage of which depends upon appropriate inhaler technique.10 Improvement of patients’ knowledge regarding inhalation technique would lead to enhanced satisfaction along with better adherence and consequently to better outcome in proper treatment of asthma.11 For inhalation drug therapy, many devices are available along with metered dose inhalers (MDIs) are the most commonly prescribed and used inhaler devices.8 A pressurized Metered Dose Inhaler (pMDI) is convenient, small in size and portable device that delivers a calculated amount of active ingredients (pharmacological agents) to lungs i.e., directly to bronchioles.12 Lack of instructions demonstration about the disease asthma and inhalers use or deficiency of regular follow-up is more likely to contribute to the inadequate use of an asthma inhaler device and consequently poor disease control with raised emergency department visits and hospitalization.13
Adherence with inhalation therapy is a basic component for respiratory disease management. But, adherence with therapy directly depends upon the satisfaction with therapy.11 Asthma management through inhalation therapy depends largely upon patient’s technique of usage of inhalers.14 Therefore, for appropriate disease control and better quality of life, health care professionals should focus on educating patients for correct inhalation technique as; it will result in enhanced satisfaction, leading to better adherence and ultimately long term disease control.11
Multiple research studies accessed patient’s inhaler satisfaction among asthma and Chronic Obstructive Pulmonary Disease (COPD) collectively by grouping them in single study group. Thus, not presenting a clear difference in inhaler satisfaction among asthma and COPD patients.15
The objective of this current cross-sectional study is to determine the asthma patient’s satisfaction with inhalers. As well as the influence of pharmacist led educational intervention upon inhaler satisfaction of asthma patients.
MATERIALS AND METHODS
Study Design and Study Subjects
This cross sectional, observational study was conducted upon asthma diagnosed adult patients from a federal hospital (PIMS) located in an urban sector of Islamabad, Pakistan. Due to well established pulmonary department, it has enhanced patient load belonging to various ethnic groups throughout the country. The research was ethically approved by the hospital’s Ethical Review Board (ERB) with the research protocol number: SZABMU/220M.
Inclusion and Exclusion criteria
The inclusion criteria for this study included physician diagnosed asthma patients with age greater than or above 18 years. Moreover, those asthma patients were included in the study that were currently using metered dose inhaler as well as using the same inhaler for the past 6 months. However, the patients with no record of current and previous inhalation therapy with MDIs were excluded from the study. The patients using nebulizers and other types of inhalers except for MDIs were excluded along with the patients who were unable to self-administer their pMDI. Informed patient consent form was received from patients before including them in the current study. The data from study subjects was maintained confidential and kept anonymous.
Sample size
According to G power calculator formula statistics, the sample size was set at two hundred and seven study subjects. The minimum sample size was 200 and 207 sample size was included. G power calculations, along with two arm proportions, α value was 0.05, β value was 0.80 and the calculated OR was 2.089 having 95% CI (Confidence Interval).
Study Procedure
The data of study subjects was recorded on a data collection form. Study subject’s demographics along with patient’s disease history were recorded from patient’s medical record file. Socio-demographic variable’s data included; Gender, age, area of residence, ethnic group, level of education, socio-economic status and assistance required during reading. Moreover, the medication related variables recorded included; duration of disease, duration of using MDIs, inhalation medications prescribed, level of instructions previously provided to patient and the frequency of using MDI. These baseline observations were recorded during the first patient visit to pulmonary department. The satisfaction of patient with inhaler was accessed utilizing the evaluation instrument- FSI-10. Afterwards, the principal investigator presented educational intervention to study subjects regarding the proper use of MDI. The intervention included demonstrating appropriate use of MDI including physical demonstration with placebo inhaler. With the interval of two months (60 months), post intervention satisfaction with inhaler was accessed during the patient’s second visit to hospital.
Evaluation Instrument
Level and extent of satisfaction of patients with their metered dose inhalers was evaluated through FSI-10 questionnaire. Legally the questionnaire was requested from its authors having copyrights16 by fulfilling legal protocols.
FSI-10 evaluated the level of satisfaction of patients with their inhaler devices. This tool contains a total of 10 questions based upon portability, ease of use, affordability, difficulties in usage and handling and overall satisfaction. Each question response was recorded in a 5 item Likert scale as “very, fairly, somewhat, not very, hardly at all” scored from 5-1 respectively. Hence, presenting a minimum score of 0=totally unsatisfied to 50=highly satisfied. FSI-10 questionnaire was translated in Urdu (native) as well. Patients individually filled this questionnaire on their own; pre and post intervention and level of satisfaction was assessed based upon criteria set by16 as: Low satisfaction if scores< 43 and high satisfaction upon scores>43.
Statistical analysis
The statistical analyzing software used for this study was SPSS, v21.0. For inferential statistics, chi square test was used to find the p-values, where the assumptions of chi-square were not met, Fisher exact test was used. The values of p<0.05 were presented as statistically significant.
RESULTS
Originally, a total of 250 adult asthmatic patients were enrolled for this study, out of which 210 patients follow up for post-intervention evaluation. However, based upon sample size calculations, 207 patients were recruited for this study.
Demographic data of study subjects is summarized in Table 1.
| Variables | Categories | Frequency(N) | Percentage (%) |
|---|---|---|---|
| Gender | Male | 103 | 49.8 |
| Female | 104 | 50.2 | |
| Age | 18-24 years | 32 | 15.5 |
| 25-44 years | 58 | 28.0 | |
| 45-64 years | 78 | 37.7 | |
| 65 and above | 39 | 18.8 | |
| Area | Rural | 116 | 56 |
| Urban | 91 | 44 | |
| Ethnicity | Punjabi | 109 | 52.7 |
| Pathan | 64 | 30.9 | |
| Others | 34 | 16.4 | |
| Education | Not Educated | 49 | 23.7 |
| Primary | 12 | 5.8 | |
| Secondary | 14 | 6.8 | |
| Matriculation | 43 | 20.8 | |
| College | 42 | 20.3 | |
| Graduation | 47 | 22.7 | |
| Socioeconomic Status | Low Class | 51 | 24.6 |
| Middle Class | 153 | 73.9 | |
| Upper Class | 3 | 1.4 | |
| Assistance Reading | Assistance Required | 93 | 44.9 |
| Assistance not Required | 114 | 55.1 |
The medication related variables as well as inhaler related factors of the study subjects are presented in Table 2.
| Variable | Category | Frequency(N) | Percentage (%) |
|---|---|---|---|
| Duration of Disease | 0-5 years | 43 | 20.8 |
| 6-10 years | 80 | 38.6 | |
| 11-15 years | 33 | 15.9 | |
| >15 years | 51 | 24.6 | |
| Duration of Using MDIs | 0-5 years | 83 | 40.1 |
| 6-10 years | 68 | 32.9 | |
| 11-15 years | 38 | 18.4 | |
| >15 years | 18 | 8.7 | |
| Inhalation Medications | Reliever | 102 | 49.3 |
| Reliever+Corticosteroids | 105 | 50.7 | |
| Instruction Methods | Never Instructed | 163 | 78.7 |
| Verbally Instructed | 43 | 20.8 | |
| Verbally Instructed+Written material provided | 01 | 0.5 | |
| Frequency of using MDI | As Needed | 167 | 80.7 |
| As Prescribed | 40 | 19.3 |
Feeling of satisfaction with inhalers- FSI-10- Pre and Post intervention are elaborated in Tables 3 and 4 consecutively. The results illustrated that majority of the patients i.e., 52.2% responded to be “Fairy satisfied” with their inhalers after they have been educated thoroughly.
| Variables (Questions) | Categories N (%) | ||||
|---|---|---|---|---|---|
| Very (5) | Fairly (4) | Somewhat (3) | Not very (2) | Hardly at all (1) | |
| 1. Has it been easy to learn how to use the inhaler? | 8 (3.9) | 39 (18.8) | 73 (35.3) | 61 (29.5) | 26 (12.6) |
| 2. Was it easy to prepare the inhaler for use? | 8 (3.9) | 43 (20.8) | 65 (31.4) | 72 (34.8) | 19 (9.2) |
| 3. Was it easy to use the inhaler? | 04 (1.9) | 34 (16.4) | 74 (35.7) | 73 (35.3) | 22 (10.6) |
| 4. Was it easy to keep the inhaler clean and in good working condition? | 14 (6.8) | 39 (18.8) | 84 (40.6) | 63 (30.4) | 07 (3.4) |
| 5. Was it easy to continue normal activities with the use of the inhaler? | 02 (1.0) | 31 (15.0) | 79 (38.2) | 69 (33.3) | 26 (12.6) |
| 6. Did the inhaler fit your lips comfortably? | 06 (2.9) | 43 (20.8) | 67 (32.4) | 78 (37.7) | 13 (6.3) |
| 7. Was using the inhaler easy in terms of size and weight? | 08 (3.9) | 90 (43.5) | 61 (29.5) | 45 (21.7) | 03 (1.4) |
| 8. Was it easy to carry the inhaler with you? | 07 (3.4) | 74 (35.7) | 73 (35.3) | 49 (23.7) | 04 (1.9) |
| 9. After you’ve used the inhaler, do you have the feeling that you used it correctly? | 02 (1.0) | 33 (15.9) | 62 (30.0) | 77 (37.2) | 33 (15.9) |
| 10. Overall, considering your responses to the previous questions, were you satisfied with your inhaler? | 03 (1.4) | 29 (14.0) | 56 (27.1) | 89 (43.0) | 30 (14.5) |
| Variables | Categories N (%) | ||||
|---|---|---|---|---|---|
| Very (5) | Fairly (4) | Somewhat (3) | Not very (2) | Hardly at all (1) | |
| 1. Has it been easy to learn how to use the inhaler? | 117 (56.5) | 55 (26.6) | 32 (15.5) | 02 (1.0) | 01 (0.5) |
| 2. Was it easy to prepare the inhaler for use? | 101 (48.8) | 66 (31.9) | 36 (17.4) | 03 (1.4) | 01 (0.5) |
| 3. Was it easy to use the inhaler? | 102 (49.3) | 63 (30.4) | 38 (18.4) | 03 (1.4) | 01 (0.5) |
| 4. Was it easy to keep the inhaler clean and in good working condition? | 86 (41.5) | 80 (38.6) | 37 (17.9) | 03 (1.4) | 01 (0.5) |
| 5. Was it easy to continue normal activities with the use of the inhaler? | 65 (31.4) | 92 (44.4) | 43 (20.8) | 06 (2.9) | 01 (0.5) |
| 6. Did the inhaler fit your lips comfortably? | 69 (33.3) | 93 (44.9) | 37 (17.9) | 07 (3.4) | 01 (0.5) |
| 7. Was using the inhaler easy in terms of size and weight? | 111 (53.6) | 59 (28.5) | 31 (15.0) | 05 (2.4) | 01 (0.5) |
| 8. Was it easy to carry the inhaler with you? | 106 (51.2) | 63 (30.4) | 31 (15.0) | 06 (2.9) | 01 (0.5) |
| 9. After you’ve used the inhaler, do you have the feeling that you used it correctly? | 101 (48.8) | 72 (34.8) | 31 (15.0) | 02 (1.0) | 01 (0.5) |
| 10. Overall, considering your responses to the previous questions, were you satisfied with your inhaler? | 60 (29.0) | 108 (52.2) | 32 (15.5) | 06 (2.9) | 01 (0.5) |
However, a large number of patients i.e., 48.8% were confident that they are using their inhaler correctly whereas, before intervention 37.2% patients believed that they do not use their inhaler correctly.
Level of Satisfaction with inhalers
Total scores were calculated by summarizing the scores of all 10 questions of FSI questionnaire. Hence, presenting a minimum score of 0=totally unsatisfied to 50=highly satisfied. Level of satisfaction with inhalers was assessed based upon criteria set by16 as: “Low satisfaction” if total scores are <43 and “High satisfaction” on scores > 43.
Majority of the asthma patients (197) i.e., 95.2% were observed to have low satisfaction regarding their pressurized meter dose inhalers. Only 4.8% patients were those who presented high satisfaction with their inhaler. However, satisfaction of patients with their inhalers was raised from 4.8% before intervention to 58.5% after intervention and study subjects presenting low satisfaction were reduced from 95.2% pre intervention to 41.5% post intervention. Intervention results in increase in high satisfaction and decrease in low satisfaction. The patient’s satisfaction with inhalers as the result of intervention is summarized in Table 5. Graphical representation of the difference observed in level of satisfaction before and after the provision of intervention is illustrated in the Figure 1.
| Variable | Categories | Pre- intervention | Post-intervention | p-value* |
|---|---|---|---|---|
| Satisfaction with Inhalers | Low satisfaction | 197 (95.2%) | 86 (41.5%) | <0.001 |
| High satisfaction | 10 (4.8%) | 121 (58.5%) |
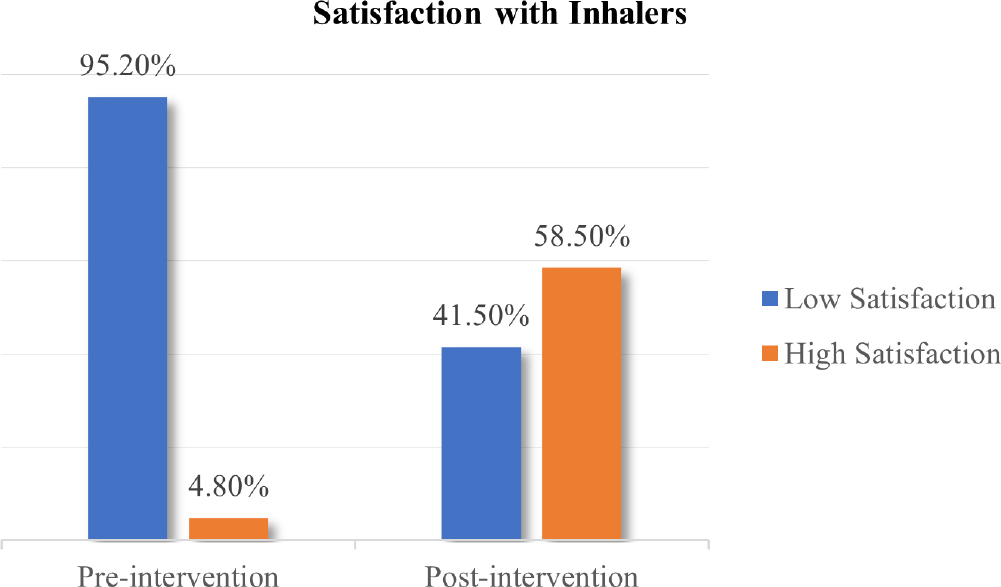
Figure 1:
Feeling of satisfaction with inhalers pre intervention and post intervention.
Statistical analysis revealed a significant increase in satisfaction of patients as the result of educational intervention (p<0.05) which indicates that instructing patients regarding meter dose inhalers resulted in increasing the level of satisfaction of patients with their inhalers.
Statistical analysis of feeling of satisfaction as the result of educational intervention is demonstrated in Table 5.
The univariate analysis of the FSI-10 questionnaire data demonstrates a noteworthy association of the intervention given to patients regarding inhaler usage with its effect on the patients’ level of satisfaction with the inhaler. Our study showed p-value of <0.001 (p<0.05) which statistically proves that there is a highly significant effect of intervention given to the patient on the use of inhaler on their level of satisfaction.
The association of demographic variables with inhaler’s satisfaction is presented in the Table 6.
| Variables | Categories | Low satisfaction N (%) | High satisfaction N (%) | p-value * |
|---|---|---|---|---|
| Gender | Male | 42 (40.78) | 61(59.22) | |
| Female | 44 (42.30) | 60 (57.69) | 0.823* | |
| Age | 18-24 years | 5 (15.6) | 27 (84.3) | |
| 25-44 years | 18 (31.0) | 40 (68.9) | <0.001* | |
| 45-64 years | 36 (46.1) | 42 (53.8) | ||
| 65 and above | 27 (69.2) | 12 (30.8) | ||
| Area | Rural | 60 (51.7) | 56 (48.3) | <0.001* |
| Urban | 26 (28.6) | 65 (71.4) | ||
| Ethnicity | Punjabi | 51 (46.8) | 58 (53.2) | 0.416* |
| Pathan | 22 (34.4) | 42 (65.6) | ||
| Others | 13 (38.2) | 21 (61.7) | ||
| Education | Not Educated | 31 (63.2) | 18 (36.7) | <0.001* |
| Primary | 4 (33.3) | 8 (66.6) | ||
| Secondary | 8 (57.1) | 6 (42.8) | ||
| Matriculation | 21 (48.8) | 22 (51.1) | ||
| College | 9 (21.4) | 33 (78.6) | ||
| Graduation | 13 (27.6) | 34 (72.3) | ||
| Socioeconomic Status | Low Class | 25 (49.0) | 26 (50.9) | |
| Middle Class | 61 (39.9) | 92 (60.1) | 0.175* | |
| Upper Class | 0 (0.0) | 3 (100.0) | ||
| Assistance Reading | Assistance Required | 53 (56.9%) | 40 (43.0%) | <0.001* |
| Assistance not Required | 33 (28.9%) | 81 (71.1%) | ||
| Duration of disease | 0-5 years | 3 (6.9) | 40 (93.0) | <0.001** |
| 6-10 years | 27 (33.7) | 53 (66.2) | ||
| 11-15 years | 19 (57.6) | 14 (42.4) | ||
| >15 years | 37 (72.5) | 14 (27.4) | ||
| Duration of using MDIs | 0-5 years | 11 (13.2) | 72 (86.7) | <0.001* |
| 6-10 years | 33 (48.5) | 35 (51.5) | ||
| 11-15 years | 26 (68.4) | 12 (31.6) | ||
| >15 years | 16 (88.8) | 2 (11.1) | ||
| Instruction methods | Never Instructed | 65 (39.8) | 98 (60.1) | 0.34* |
| Verbally Instructed | 21 (48.8) | 22 (51.2) | ||
| Verbal+Written material provided | 0 (0) | 1 (100) | ||
| Frequency of using | As Needed | 74 (44.3%) | 93 (55.7%) | 0.099* |
| MDIs | As Prescribed | 12 (30.0%) | 28 (70.0%) |
DISCUSSION
The present study, investigated the effect of pharmacist involvement upon feeling of satisfaction with inhaler among asthma patients. The assessment of patient satisfaction was performed using self-completed questionnaire i.e., the FSI-10. The patients found the FSI-10 questionnaire to be easily comprehensible and were able to complete it without difficulty. To our understanding, there has been no previous research conducted in a standardized manner to assess patient satisfaction with inhaler devices using questionnaire FSI-10 among the population in Pakistan. Therefore, the present research study was conducted to access patient satisfaction with their inhalers. Because, the satisfaction with therapy is observed to be directly associated with adherence with inhalation therapy.17 Somehow similar number of male and female asthma patients i.e., 49.8% and 50.2% were recruited for this study. 55.1 % of them did not require assistance reading the questionnaire. Among which majority of the patients i.e., 78.7% were never instructed regarding the inhaler use.
According to the statistical analysis on the data collected from the patients before intervention if we group the 5-point scale responses of the patient to positive (very satisfied, fairly or somewhat satisfied) and negative (not very or hardly satisfied) responses, 42.1% patient responded negative in ease of learning to use the inhaler (item-1). These results are in contrast to the study conducted in Barcelona, Spain where majority of the asthma patients (54.7%) presented positive response in ease of learning their inhaler technique.18
However, as the result of intervention the satisfaction of the patients (very or fairly satisfied) regarding the ease of learning to use their inhaler improved to 83.1% in the present study.
The justification behind significant negative response on ease of learning to use the inhaler is most of the patients enrolled for current study i.e., 56% were from rural areas and 23.7% were illiterate. So, they find it difficult to learn the use of inhaler. In contrast, the Spanish population presented positive response i.e., ease to learning inhaler technique that might be due to their enhanced literacy rate.19
The satisfaction of patients regarding the ease to prepare inhaler for use (item-2) was 24.7% i.e., very or fairly satisfied. But it was enhanced to 80.7% as the result of educational intervention. However, a recent study conducted in accordance with Declaration of Helsinki in Spain (Barcelona) presented somewhat different results. The majority of Spanish asthmatic patients (57.6%) found it very easy to prepare inhaler for use.18 The possible reason of finding it difficult to prepare inhaler for use could be the lack of inhaler technique training from the healthcare professionals.
During baseline survey, only 18.54% patients find it very or fairly easy to use to their inhaler (item-3) whereas, 81.45% patients didn’t find it easy to use the inhalers. The intervention proved helpful in enhancing the satisfaction of patients regarding the ease to use their inhaler. As the result, 79.73% patients presented that they find it very or fairly easy to use their inhaler. In contrast, the research conducted upon 406 asthmatic Spanish adults presented that majority (62.1%) of the participants find it easy to use their inhaler during baseline survey.18 This might be because of the better inhaler technique in Spanish patients that leads to ease of inhaler use.16
During baseline survey, majority of the study subjects presented poor satisfaction regarding ease to keep the inhaler clean, continuing normal routine activities with inhaler use, unsatisfaction regarding shape, size and weight of inhaler as well as carrying inhaler with themselves. The probable reason could be the fact that majority of patients recruited for the study were not using inhalers as prescribed. In fact, majority of the study subjects preferred using inhalers as needed i.e., 80.7%.
Similarly, 16.91% patients felt that they use their inhaler correctly (item-9). However, after intervention it was enhanced to 83.6%.
The possible reason could be the lack of guidance regarding use of inhalers as 78.7% patients presented that they were never instructed about appropriate inhaler use. Previous studies from Pakistan has also confirmed the lack of inhaler technique instructions given to patients.8
In conclusion, only 15.41% patients presented overall satisfaction with their inhaler (item-10). That was enhanced to 81.21% as the result of pharmacist led educational intervention. The reason behind unsatisfaction with inhalers at baseline could be the feeling of inappropriate use of inhalers. As majority of the patients i.e., 83.09% felt that they did not use their inhaler correctly. That might have led to unsatisfaction with their inhaler. In contrast, a study conducted in Sydney, Australia under the approval of University of Sydney Human-Research-Ethics-Committee presented higher satisfaction of Australian population with their inhalers.20 Another study conducted on Spanish patients recruited from 9 different hospitals presented similar results i.e., most of the participants well accepted their inhalers (presented raised satisfaction at baseline).16
The possible reason could be the effective patient counselling in the community pharmacies of developed countries by pharmacists upon medication dispensing, that contributed towards raised patients’ satisfaction with their inhalers.21
The baseline survey presented that out of the observed patients the majority i.e., 95.2% exhibited a low level of satisfaction. These results are in accordance with the study conducted in fifty-nine hospital setups of Spain, where the patients presenting high satisfaction with MDIs were 27.9%.15 The intervention resulted in a significant increase in patient satisfaction with their inhalers, with the percentage rising from 4.8% before the intervention to 58.5% after the intervention. The proportion of patients expressing low satisfaction decreased significantly, dropping from 95.2% before intervention to 41.5% after intervention. The probable reason could be the enhanced satisfaction of patients with the increase in knowledge regarding inhaler technique. It has been proved in the previous studies that inhaler technique of patients could be improved as the result of counselling and educational intervention.22
In the present study, no statistically significant association was observed between gender and inhaler satisfaction of patients. Similarly, a prospective cross sectional study conducted in Daegu upon 261 South Korean patients, in hospital settings of Yeungnam University presented no statistically significant association between gender and patient’s inhaler satisfaction.23
However, a prospective cross-sectional study conducted upon 800 Spanish adults, presented somewhat contrary results i.e., male patients being slightly more satisfied with their inhalers as compared to the female patients.19 Similarly, another study conducted on fifty nine hospitals across Spain, upon 778 asthmatic patients resulted that male patients are slightly more inclined towards high inhaler satisfaction.22 The probable reason could be the greater literacy rate of male population as compared to female population.24
According to the current study, age of patients was associated with the level of satisfaction presented by patients. The results presented that the younger age group of patients i.e., 18-24 years old patients depicted higher satisfaction as compared to patients with higher age, especially old age patients. The probable reason would be the enhanced learning abilities of young people, as cognitive and learning abilities of people decline with age.25 Therefore, better response of educational intervention in terms of satisfaction with inhaler was observed in younger patients.
CONCLUSION
The study demonstrated a significant increase in patient satisfaction with inhalers when pharmacists were involved in educating them about inhalers. This finding suggests that pharmacist interventions, such as education and counseling, play a vital role in improving patient satisfaction and overall management of asthma. Patients who received proper instructions on inhaler technique and usage reported higher levels of satisfaction. This emphasizes the need for pharmacist-led interventions to address knowledge gaps and ensure optimal use of inhaler devices.
It was observed after the statistical analysis on the data collected using FSI-10 questionnaire that tailoring counseling sessions to individual patient needs contributed to increased satisfaction. When pharmacists took the time to understand each patient’s unique circumstances and preferences, they could provide personalized recommendations and address concerns effectively. The present study revealed that patients who received ongoing support from the same pharmacist reported higher satisfaction levels. Continuity of care allows pharmacists to develop a deeper understanding of patients’ needs, monitor their progress, and provide consistent guidance. This finding highlights the importance of establishing long-term relationships between patients and pharmacists to ensure sustained satisfaction.
Cite this article
Shahid S. The Effect of Pharmacist Involvement Upon the Satisfaction with Inhalers (FSI-10) among Asthma Patients. J Young Pharm. 2024;16(1):115-23.
ACKNOWLEDGEMENT
The author would like to acknowledge the ethical review board of “Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad” for approving the current study protocol. Moreover, the study participants who voluntarily enrolled for the present study project are sincerely acknowledged.
The author would like to acknowledge the ethical review board of “Shaheed Zulfiqar Ali Bhutto Medical University, Islamabad” for approving the current study protocol. Moreover, the study participants who voluntarily enrolled for the present study project are sincerely acknowledged.
References
- Against Shamkuwar CA, Kumari N, Meshram SH, Dakhale GN, Motghare VM. Evaluation of Knowledge, attitude and medication adherence among asthmatics outpatients in tertiary care teaching hospital-A questionnaire-based study. J Young Pharm. 2016;8(1):39-43. [CrossRef] | [Google Scholar]
- Ngo CQ, Phan DM, Vu GV, Dao PN, Phan PT, Chu HT, et al. Inhaler technique and adherence to inhaled medications among patients with acute exacerbation of chronic obstructive pulmonary disease in Vietnam. Int J Environ Res Public Health. 2019;16(2):185 [PubMed] | [CrossRef] | [Google Scholar]
- Iqbal MS, Al-Saikhan FI, Iqbal MZ, Ahmed NJ. The burden of illness of acute exacerbation of asthma. Asian J Pharm. 2020;14:183-7. [PubMed] | [CrossRef] | [Google Scholar]
- Iqbal MS, Al-Saikhan FI, Ahmed NJ, Iqbal MZ. How do out-of-pocket expenditures affect healthcare: A qualitative insight of acute exacerbation among asthma patients. J Pharm Res Int. 2020;32:67-73. [CrossRef] | [Google Scholar]
- Lalani N. A study of knowledge assessment and competence in asthma and inhaler technique of nurses employed at university teaching hospital. the. Health. 2012;3:16-8. [CrossRef] | [Google Scholar]
- Burney P, Jarvis D, Perez-Padilla R. The global burden of chronic respiratory disease in adults. Int J Tuberc Lung Dis. 2015;19(1):10-20. [PubMed] | [CrossRef] | [Google Scholar]
- Hardwell A, Barber V, Hargadon T, McKnight E, Holmes J, Levy ML, et al. Technique training does not improve the ability of most patients to use pressurised metered-dose inhalers (pMDIs). Prim Care Respir J. 2011;20(1):92-6. [PubMed] | [CrossRef] | [Google Scholar]
- Shahid S, Ahmed F, Bajwa A, Ans M, Sana A, Abbas S, et al. The impact of an educational intervention on the skill of community pharmacists in the use of a pressurized metered-dose inhaler: A covert simulated patient approach in Pakistan. Int J Pharm Investig. 2022;12(3):380-5. [CrossRef] | [Google Scholar]
- Iqbal MS, Al-Saikhan FI, Ahmed NJ, Iqbal MZ. Pharmacoeconomic analysis of acute exacerbation of chronic obstructive pulmonary disease. Int J Pharm Investig. 2020;32(4):59-66. [CrossRef] | [Google Scholar]
- Mubarak N, Hatah E, Khan TM, Zin CS. A systematic review and meta-analysis of the impact of collaborative practice between community pharmacist and general practitioner on asthma management. J Asthma Allergy. 2019;12:109-53. [PubMed] | [CrossRef] | [Google Scholar]
- Dudvarski Ilic AD, Zugic V, Zvezdin B, Kopitovic I, Cekerevac I, Cupurdija V, et al. Influence of inhaler technique on asthma and COPD control: a multicenter experience. Int J Chronic Obs Pulmon Dis. 2016(11):2509-17. [CrossRef] | [Google Scholar]
- Iqbal MS, Al-Saikhan FI, Iqbal MZ, Ahmed NJ. The burden of illness of acute exacerbation of asthma. Asian J Pharm. 2020;14(2):183-7. [CrossRef] | [Google Scholar]
- Ahmed A, Al-harbi A, Khan M, Baharoon S, Salih SB. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Al-jahdali H. Allergy Asthma Clin Immunol. 2013:1 [CrossRef] | [Google Scholar]
- Ali HD, Worku GS, Alemayehu AA, Gebrehiwot WH. Competence in metered dose inhaler technique among dispensers in Mekelle. Allergy Asthma Clin Immunol. 2014;10(1):18 [PubMed] | [CrossRef] | [Google Scholar]
- Plaza V, Giner J, Calle M, Rytilä P, Campo C, Ribó P, et al. Impact of patient satisfaction with his or her inhaler on adherence and asthma control. Allergy Asthma Proc. 2018;39(6):437-44. [PubMed] | [CrossRef] | [Google Scholar]
- Tordera MP, Viejo JL, Sanchos J, Badia X, Cobos N, Picado C, et al. Assessment of patient satisfaction and preferences with inhalers in asthma with the FSI-10 Questionnaire. Arch Bronconeumol. 2008;44(7):346-52. [CrossRef] | [Google Scholar]
- Rogueda P, Traini D. Expert Review of Respiratory Medicine The future of inhalers: how can we improve drug delivery in asthma and COPD?. Expert Rev Respir Med. 2016;10(10):1041-4. [PubMed] | [CrossRef] | [Google Scholar]
- Plaza V, Giner J, Curto E, Alonso-Ortiz MB, Orue MI, Vega JM, et al. Determinants and differences in satisfaction with the inhaler among patients with asthma or COPD. J Allergy Clin Immunol Pract. 2020;8(2):645-53. [PubMed] | [CrossRef] | [Google Scholar]
- Valero A, Ribó P, Maíz L, Barbero E, Calle M, Campo C, et al. Asthma patient satisfaction with different dry powder inhalers. Expert Rev Respir Med. 2019;13(2):133-8. [PubMed] | [CrossRef] | [Google Scholar]
- Jahedi L, Downie SR, Saini B, Chan HK, Bosnic-Anticevich S. Inhaler technique in asthma: how does it relate to patients’ preferences and attitudes toward their inhalers?. J Aerosol Med Pulm Drug Deliv. 2017;30(1):42-52. [PubMed] | [CrossRef] | [Google Scholar]
- Putman B, Coucke L, Vanoverschelde A, Mehuys E, Lahousse L. Community pharmacist counseling improves adherence and asthma control: a nationwide study. BMC Health Serv Res. 2022;22(1):112 [PubMed] | [CrossRef] | [Google Scholar]
- Shahid S, Ahmed F, Shahnaz G, Saqlain M, Ans M, Sana A, et al. The Impact of Theoretical and Practical Guidance regarding Metered dose Inhaler Technique on Asthma Patients. J Young Pharm. 2022;14(3):327-32. [CrossRef] | [Google Scholar]
- Jang JG, Chung JH, Shin KC, Jin HJ, Lee KH, Ahn JH, et al. Comparative study of inhaler device handling technique and risk factors for critical inhaler errors in Korean COPD patients. Int J Chron Obstruct Pulmon Dis. 2021;16:1051-9. [PubMed] | [CrossRef] | [Google Scholar]
- Houts PS, Witmer JT, Egeth HE, Loscalzo MJ, Zabora JR. Using pictographs to enhance recall of spoken medical instructions II. Patient Educ Couns. patient ed. 2001;43(3):231-42. [PubMed] | [CrossRef] | [Google Scholar]
- Turan O, Turan PA, Mirici A. Parameters affecting inhalation therapy adherence in elderly patients with chronic obstructive lung disease and asthma. Geriatr Gerontol Int. 2017;17(6):999-1005. [PubMed] | [CrossRef] | [Google Scholar]