ABSTRACT
Background
Vitiligo vulgaris is an autoimmune de-pigmentary disorder characterized by skin depigmentation that can be localized or generalized, due to destructed melanocytes. It carries a majority of stigma and has a negative impact on patient’s psychological well-being. Hence, to determine the impact of clinical pharmacist intervention on depression levels and quality of life in vitiligo patients is of utmost importance.
Materials and Methods
A prospective study in Dept. of Dermatology at a tertiary care hospital was carried out after getting ethics committee approval. Vitiligo patients aged >18 years were included. The QIDS-SR16 (Quick Inventory Depression Symptomology-Self Rating Scale) and VIS-22 (Vitiligo Impact Scale-22) scales were used to determine depression level and quality of life, respectively.
Results
Among 62 patients enrolled in the study, 64.52% were female and 35.48% were male. At the baseline, the mean VIS-22 and QIDS-SR16 scores were 15.02 and 4.92 respectively. After the pre and post evaluation of VIS-22 and QIDS-SR16, a significant percentage of difference from the baseline data to the follow-up of approximately 40.64% in VIS-22 and 53.27% in QIDS SR16 was observed.
Conclusion
The findings of this study indicate that, in addition to pharmacological therapy, appropriate counseling and general education can aid in enhancing their psychosocial behavior and quality of life and help improve the negative stigmatization in society.
INTRODUCTION
Vitiligo is an acquired autoimmune illness of the skin and mucous membranes, characterised by well-defined, depigmented macules and lesions caused by the selective loss of melanocytes. Vitiligo has an unknown aetiology and is distinguished by the depigmentation of the body’s largest organ, the skin. The estimation of the prevalence of this illness, commonly known as leukoderma in India, was between 25% and 4% across various studies and up to 8.8% in Gujarat and Rajasthan, which had the highest prevalence in the world.1
Due to the stark contrast, skin depigmentation is unmistakably distinguishable; it naturally attracts stigma in society, particularly in patients with skin of colour or a dark complexion. This social stigma leads to the impairment of psychosocial health and well-being.2,3 They draw widespread attention from the broader populace, notably whispered remarks, animosity, and ostracism.
Men, women, and children with vitiligo experience serious psychological and social challenges in India and internationally. Unfortunately, vitiligo is related to various religious beliefs in India. According to several Indian religious writings that believe in reincarnation, people who committed “Guru Droh” in their former life suffer from vitiligo in this life. This stigmatisation was observed throughout our study. Misconceptions about cuisine included the belief that eating sour foods and non-vegetarian food would increase the lesions. It is especially severe in the case of young women and children. Depression of a more severe nature was significantly more prevalent among the younger generation, the single, those with little education, and those who had the disease for a shorter period of time. Around 54.5% of Vitiligo patients suffer from depression and have diminished QoL.4
According to a recent study, people with visible vitiligo lesions on their upper extremities have a lower quality of life, indicating poor psychosocial health. Recent literature has shown that lesions on visible or exposed areas of the body show a higher Dermatology Life Quality Index (DLQI) rating than those who do not.5 Therefore, due to an unforeseeable development in the condition, the individual suffers from a negative psychosocial influence.6 Because dermatological conditions are more visibly visible, stigmatization naturally follows. Accumulation of this information was achieved through the Quick Inventory of Depressive Symptomology-Self Rating 16 (QIDS-SR16) for depression and the Vitiligo Impact Scale 22 (VIS-22) to evaluate the impairment in Quality of Life (QOL).
Since the physicians find it strenuous to monitor the individual’s psychosocial difficulties, we have tried to analyse the grey zone in the individual’s life and provide necessary counseling, therefore trying to cease the aforementioned difficulties.7 With all of these concerns about the relevance of illness progression to psychosocial imbalance in mind, there is an urgent need for health care providers to address them. In this study, we try to acknowledge, recognize, and evaluate the impairment that vitiligo has caused in the individual’s lifestyle. Hence, the present study is planned to assess the pre-and post-counselling outcome in vitiligo patients using Quick Inventory of Depressive Symptomology-Self Rating 16 (QIDS-SR16) and to assess the pre- and post- counselling outcome in vitiligo patients for Quality of life (QOL) using Vitiligo Impact Scale (VIS-22).
MATERIALS AND METHODS
Study design and sample calculation
A pre- and post-interventional study was conducted at the Department of Dermatology, KLE’s Dr. Prabhakar Kore Charitable Hospital, Nehru Nagar, Belagavi, and was approved by institutional ethical clearance (reference number: KLE/ COP/2021-22/674). The data was collected over a period of five months. Statistical data was calculated over a one-month period (December 2021-May 2022). Patients aged 18 or older, patients who agreed to participate in the study, were included in the study and patients receiving oncotherapy, and pregnant women were excluded from the study. An informed consent form was obtained from patients, and an information sheet was given in their regional language. Patients who met the inclusion criteria and participated in the study were pre-assessed for depression and quality of life using the QIDS-SR16 and VIS-22 questionnaires. After assessing the patient, an intervention was provided by the clinical pharmacist at regular intervals through counselling and a validated patient information leaflet. A three-month follow-up was followed. There was no loss of follow-up. The sample size was calculated using the universal sampling technique. Flow-chart of the study is depicted in Figure 1.
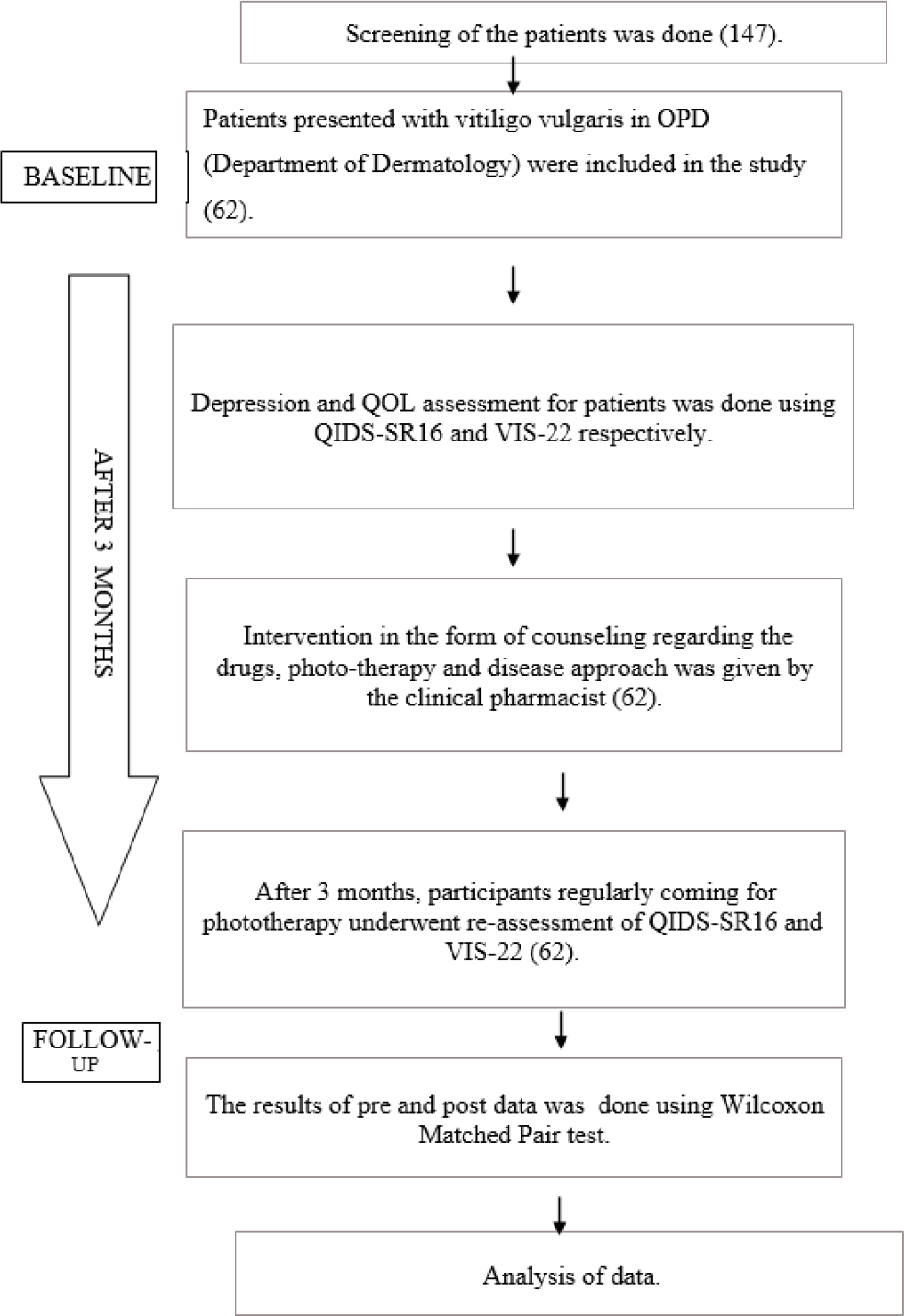
Figure 1:
Schematic diagram.
Depression Status
The level of depression in the patient was assessed using Quick Inventory Depressive Symptomology- Self Rating 16 scale developed by AJ RUSH at 2006.8 This questionnaire has six domains comprising of sad mood, concentration, energy, interest, guilt, suicidal ideation or intent. The score range for QIDS-SR16 ranges from 0 to 27, indicating no depression for score 5 or lower, mild depression indicating between 6 to 10, moderate depression indicating between 11 to 15, severe depression indicating between severe depression and a total score greater than 21 reflecting of severe depression.
Quality of Life
Quality of Life was assessed using a disease-specific questionnaire, i.e., the Vitiligo Impact Scale-22 (VIS-22), designed by V. Gupta in the year 2019. VIS-22 has 22 questions that include an array of topics, including attitude (questions 1, 4, 17, 19), anxiety (2, 11), social interactions (3, 12, 13), self-confidence (5, 18), depression (6, 9, 10, 14), treatment (7, 15, 16), family (8), marriage (20), occupation (21) and work or education (22). These are the potential scores for each question: 0 for not at all, 1 for a little, 2 for a lot, and 3 for very much. The total score goes from 0 to 66, with larger scores indicating a larger effect on life.
Intervention
All the patients enrolled in the study were assessed regularly during their follow-up visits at the dermatology department and telephonically. Based on the assessment and treatment regimen, the clinical pharmacist provided pharmaceutical care. This included the management of the disease, side effects and precautions of PUVA (Psoralen and Ultraviolet A therapy) and medications, lifestyle modifications, and general education about the disease and its effects on an individual’s psychological health. During patient education, Patient Information Leaflets (PIL’s) were also provided.
Data collection
The demographic data, subjective evidence, objective evidence, and treatment plan were compiled using Google Forms, and written consent was obtained from the patients. The questionnaire was provided to them on the Google forms and was filled out by them accordingly.
Statistical Analysis
The data was entered into an excel spreadsheet and analyzed using SPSS (IBM version 23). Comparison of pre and post scores of QIDS-SR16 and VIS-22 was done using dependent t-test.
Outcomes
Considering the obstruction caused by extent of lesion and its consequence on psychosocial health and quality of life being hampered regardless of age, sex, and disease decreases overall psychosocial health and quality of life, which will be a valuable assessment in vitiligo patients after providing counseling.
RESULTS
Comparison of baseline and follow-up data
The comparison of the description scale, pre and post was performed using paired dependent t-test methodology as shown in Figures 2 and 4. The mean difference from the baseline to the follow-up for QIDS-SR16 is 3.42 and VIS-22 is 4.28 as shown in Table 2.
| Demographic profile | No. of patients | % of patients |
|---|---|---|
| Gender | ||
| Male | 22 | 35.48 |
| Female | 40 | 64.52 |
| Age groups | ||
| 18-25 years | 13 | 20.97 |
| 26-33 years | 15 | 24.19 |
| 34-41 years | 6 | 9.68 |
| 42-49 years | 15 | 24.19 |
| 50-57 years | 4 | 6.45 |
| 58-69 years | 6 | 9.68 |
| 70-80 years | 3 | 4.84 |
| Marital status | ||
| Married | 42 | 67.74 |
| Unmarried | 20 | 32.26 |
| Total | 62 | 100.00 |
| Variables | Mean | SD | Mean difference | Percentage of difference | |
|---|---|---|---|---|---|
| QIDS SR 16 | Pre Post | 6.42 3.0 | 3.64 2.469 | 3.42 | 53.27% |
| VIS 22 | Pre Post | 14.85 10.565 | 7.254 5.78 | 4.28 | 28.85% |
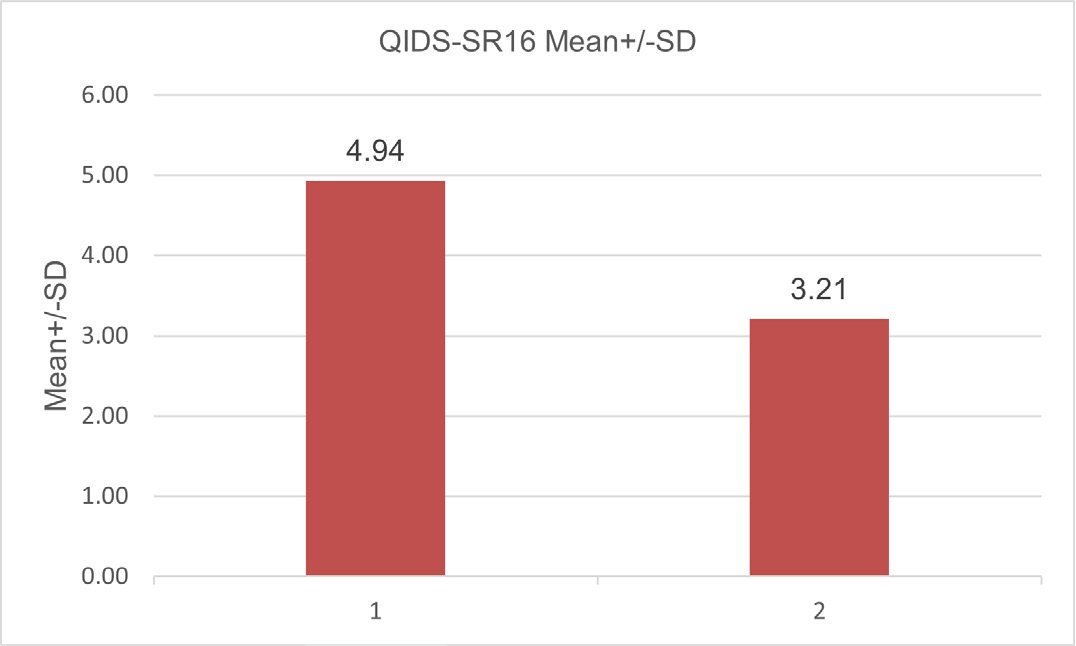
Figure 2:
The comparison of mean baseline data and mean follow-up data of QIDS-SR16.
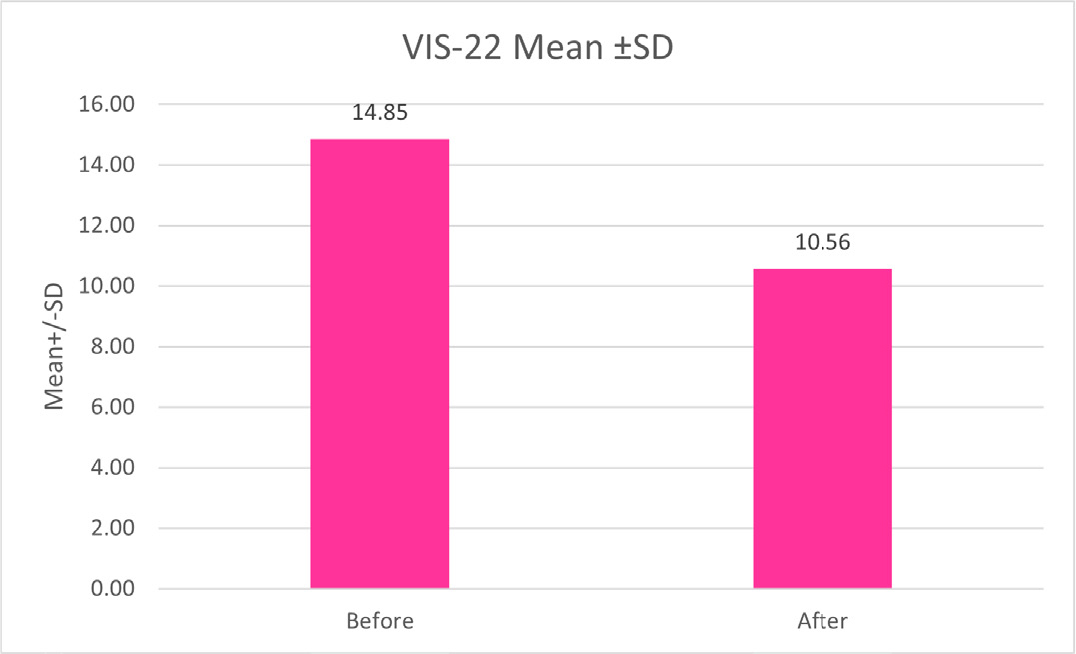
Figure 4:
The comparison of mean baseline data and mean follow-up data of VIS-22.
Comparison of depression domains
A comparative analysis for pre and post data was done using Wilcoxon matched pair t-test through which it was observed that 61.2% patient had no depression at the baseline evaluation which increases to 80.64% at the follow-up evaluation as shown in Figure 3. 32.2% patients had mild depression which decreased to 17.47% and 4.83% have had moderate depression which was reduced to 1.61% and 1.61% patient having severe depression decreased to 0 percent. Hence indicating that good number of patients having mild to moderate depression progressed to no depression and patients having severe depression progressed to moderate depression.
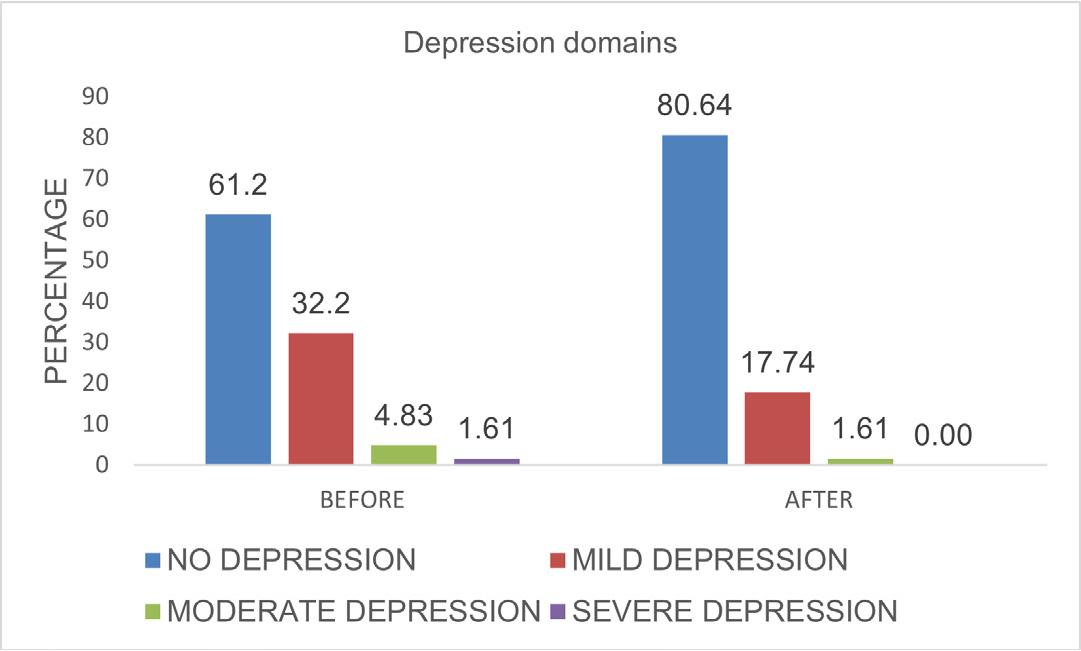
Figure 3:
Comparison of pre and post-depression based on severity of depression.
Impact on quality of life
The comparison of quality of life in patients, pre- and post-data was done using the dependent t test methodology. The mean of VIS-22 before the baseline period was 14.85±7.25, and after follow-up, the mean was estimated to be 10.56±5.78 (Figure 4). The pre-post evaluation showed that the moderate effect category had an improvement of 22.58% followed by mild effect category had an improvement of 17.54%, no effect category showed 8,87% and large effects showed 4.84% advancements at the follow-up (Figure 5). This suggests that life quality improved significantly after receiving counseling.

Figure 5:
Comparison of pre and post- quality of life based.
DISCUSSION
Vitiligo, being a de-pigmentary disorder of the skin has majorly caused a huge toll on the psychosocial behavior and emotional impact on an individual, especially living in a society where everyone’s opinion matter. Prasad et al., reported the same suggesting that the stigmatization in the Asian culture is increasing.7
The total number of 62 patients recruited for the study (Table 1), with the majority (64.52%) being female and the remainder (35.48%) being male. These findings slightly matched those of Pahwa et al. and Salzes et al., in which 65.7% and 62% of participants were females, respectively, and 34.3% and 38% of participants were men.9,10 Although the majority of participants in studies by Pahwa et al. and Wang et al. were men, the participants in this study ranged in age from 18 to 80 years, with the majority falling between the ages of 26 and 33 and 42 and 49.10,11 Additionally, more than half of them (67.74%) were married.
Tacrolimus topical ointment was highly prescribed to 73.8% patients followed by narrowband UV-B phototherapy was received by 59% of patients. In the category of oral immunosuppressant, tablet Azoran 50 mg was received 34.4% and corticosteroid, tablet betamethasone 1mg was received by 45.9%. The extent of the lesion size was calculated using Vitiligo Extent Tensity Index (VETI) where the mean of baseline assessment of the lesion extent was found out to be 60.69 and after receiving continuous pharmacological and regular phototherapy session, a decrease in vitiligo lesions was observed to be at 53.61 mean values. It was observed that the patients who were regular for phototherapy had quicker re-pigmentation of the depigmented lesions compared to those who were irregular in receiving their treatment.
All patients received constant words of support and encouragement from the clinical pharmacist at their follow-up visits in the dermatology Outpatient Department (OPD) for about 3 months. After completion of about 3 months of receiving treatment and counseling, a follow-up of QIDS-SR16 scale was re-done again. It was found that there was a significant drop in the depression level of in terms of sad mood reduced from 69.04% to 52.38% in married individuals, whereas it remained unchanged in unmarried individuals. In the sleep disturbance domain unmarried individuals improved from 27.41% to 19.35% and married individuals remained unchanged. Stress is directly linked to mood swings and sleep pattern12 hence degrading the health of the skin as stress aggravates vitiligo frequently and for some of us, just knowing this can make us feel more worried.
The mean VIS score in this study was 14.85±7.24 (Table 1), which was higher than that reported by Kota et al. (mean 7.02) but lower than Aarzoo Pahwa et al. (mean 26.48).10,13 The average mean of VIS-22 in our study was higher in females compared to males, which is 15.90 and 13.79, respectively, which is similar to several studies.9–11 This higher impairment in women is most likely due to greater social stress as a result of societal prejudice as well as greater concern for their appearance. After establishing a connection with the patient and providing them with adequate counseling, a difference in quality of life was seen. An impact of 22.58% was seen on the moderate effect of QOL, and on the large effect, the difference was 4.84%. Using VIS-22 we found majority of patients were worried of developing new lesions followed by patients worried about wearing their choice of clothes in public and feeling helpless about the disease.
However, a number of patients continued to have a mild effect on QOL, which may be due to the psychological impact caused by vitiligo, which takes time to heal. The development of visible skin lesions and their constant progression may have a substantial negative impact on patient’s QOL in terms of their health and psychiatric morbidity may develop as a side effect. Although vitiligo is seen as a cosmetic issue it has a significant impact on patient’s QOL and their psychological wellbeing.
Early on in the treatment course of the disease, offering these patients psychological support can assist them in accepting their condition and minimising its social impact. A constant reminder of the fact that this de-pigmentary disorder, which has major effects on the cosmetological appearance of an individual, has nothing to do with their potential as individuals or their view of themselves as worthwhile was persistently given. As a result, assisting them in improving their sleep cycle, decision-making abilities, and overall well-being will make them less restless and more confident.
The results of this study emphasize a very good improvement from the baseline to the follow-up. This clearly demonstrates that clinical pharmacists have a positive impact on patient counselling (interventions performed and patient information leaflets provided). Additionally, it can also increase medication compliance, which will enhance how the sickness will manifest.14 The use of pharmaceutical care services for patients with vitiligo who have impairments and poor psychosocial health improves their condition, reduces side effects, and improves the patients’ quality of life.15 The effectiveness of therapy may be improved by dermatologists and pharmacists working collaboratively as well as by actively including patients and their families in the therapeutic process. Vitiligo vulgaris requires lifelong management; hence, seeking treatment for a longer duration of time requires better adherence to the treatment, which is faced as a major challenge. We have tried to overcome this challenge, thereby improving psychosocial behaviour and quality of life.16
Limitation
- This study needs to be carried out for a longer duration to observe for a longer period.
- The total duration of this study was 6 months hence more number of follow-ups could not done.
- Our study may not show the impact of an intervention on people who do not seek treatment in the Department of Dermatology.
CONCLUSION
The findings of this study indicate that, in addition to pharmacological therapy, appropriate counseling and general education can aid in enhancing their psychosocial behavior and quality of life and help improve the negative stigmatization in society. The present study could serve as a springboard for initiating methodological guidelines for providing pharmacological treatment services to depressed patients. The viability of implementing community-based pharmacological therapy for vitiligo patients with depression will need to be evaluated by a number of follow-up studies.
Cite this article
Yadav S, Hiremath A, Sequeira J, Roy A, Jose A, Doshi B, et al. Clinical Pharmacist Intervention on the Quality of Life and Psychosocial Health in Patients with Vitiligo Vulgaris: A Prospective Study. J Young Pharm. 2024;16(1):124-9.
ACKNOWLEDGEMENT
We would like to thank the Principal of KLE College of Pharmacy, Head of Department of Pharmacy Practice, KLE’s Dr. Prabhakar Kore Hospital and Medical Research Centre, Belagavi, Superintendent of KLE’s Dr. Prabhakar Kore Hospital, Belagavi, MD of KLE’s Dr. Prabhakar Kore Hospital, Belagavi and Head of Department of Dermatology and Venereology.
We would like to thank the Principal of KLE College of Pharmacy, Head of Department of Pharmacy Practice, KLE’s Dr. Prabhakar Kore Hospital and Medical Research Centre, Belagavi, Superintendent of KLE’s Dr. Prabhakar Kore Hospital, Belagavi, MD of KLE’s Dr. Prabhakar Kore Hospital, Belagavi and Head of Department of Dermatology and Venereology.
ABBREVIATIONS
| QIDS-SR16 | Quick Inventory Depression Symptomology-Self Rating Scale |
|---|---|
| VIS-22 | Vitiligo Impact Scale-22 |
| DLQI | Dermatology Life Quality Index |
| QOL | Quality of Life |
| OPD | Outpatient department |
| PUVA | Psoralen and Ultraviolet a Therapy |
| PIL | Patient information leaflet |
| VETI | Vitiligo Extent Tensity Index |
References
- Alikhan A, Felsten LM, Daly M, Petronic-Rosic V. Vitiligo: a comprehensive overview: part I [introduction]. J Am Acad Dermatol. 2011;65(3):473-91. [PubMed] | [CrossRef] | [Google Scholar]
- Lai YC, Yew YW, Kennedy C, Schwartz RA. Vitiligo and depression: a systematic review and meta-analysis of observational studies. Br J Dermatol. 2017;177(3):708-18. [PubMed] | [CrossRef] | [Google Scholar]
- Papadopoulos L, Bor R, Legg C. Coping with the disfiguring effects of vitiligo: a preliminary investigation into the effects of cognitive behavioural therapy. Br J Med Psychol. 1999;72(3):385-96. [PubMed] | [CrossRef] | [Google Scholar]
- Benzekri L, Ezzedine K, Gauthier Y. Vitiligo Potential Repigmentation Index: a simple clinical score that might predict the ability of vitiligo lesions to repigment under therapy. Br J Dermatol. 2013;168(5):1143-6. [PubMed] | [CrossRef] | [Google Scholar]
- Ezzedine K, Eleftheriadou V, Jones H, Bibeau K, Kuo FI, Sturm D, et al. Psychosocial effects of vitiligo: A systematic literature review. Am J Clin Dermatol. 2021;22(6):757-74. [PubMed] | [CrossRef] | [Google Scholar]
- Kostopoulou P, Jouary T, Quintard B, Ezzedine K, Marques S, Boutchnei S, et al. Objective vs. subjective factors in the psychological impact of vitiligo: the experience from a French referralcentre. Br J Dermatol. 2009;161(1):128-33. [PubMed] | [CrossRef] | [Google Scholar]
- Parsad D, Kumarasinge SP. Psychosocial implications of pigmentary disorders in Asia. PASPCR Comment. 2006;1:1-8. [PubMed] | [CrossRef] | [Google Scholar]
- Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein DN, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol Psychiatry. 2003;54(5):573-83. [PubMed] | [CrossRef] | [Google Scholar]
- Belgaumkar VA, Chavan RB, Deshmukh NS, Warke NV. Impact of vitiligo on quality of life: A cross-sectional pilot study from Western India. J Skin Stem Cell. 2020;30(Array):7 [CrossRef] | [Google Scholar]
- PAHWA A, RATHORE PK. Assessment of impact of vitiligo and its distribution on psychosocial life: A cross-sectional study. J Clin Diagn Res. 2022;16(2) [CrossRef] | [Google Scholar]
- Wang KY, Wang KH, Zhang ZP. Health-related quality of life and marital quality of vitiligo patients in China. J Eur Acad Dermatol Venereol. 2011;25(4):429-35. [PubMed] | [CrossRef] | [Google Scholar]
- Silverberg JI, Silverberg NB. Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol. 2013;149(2):159-64. [PubMed] | [CrossRef] | [Google Scholar]
- RAO NN, THOMBRE RA, AHMAD A. Correlation of dermatology life quality index and vitiligo extent tensity index: A cross-sectional study. J Clin Diagn Res. 2022;16(12) [PubMed] | [CrossRef] | [Google Scholar]
- Pahwa P, Mehta M, Khaitan BK, Sharma VK, Ramam M. The psychosocial impact of vitiligo in Indian patients. Indian J Dermatol Venereol Leprol. 2013;79(5):679-85. [PubMed] | [CrossRef] | [Google Scholar]
- Hiremath AC, Bhandari R, Wali S, Ganachari MS, Doshi B. Impact of clinical pharmacist on medication adherence among psoriasis patients: A randomized controlled study. Clin Epidemiol Glob Health. 2021;10(10):100687 [CrossRef] | [Google Scholar]
- Joshi A, Joshy J, Mathew KA, Jain SR, Hiremath AC, Tekkalaki BV, et al. Quality of life in Schizophrenia patients with and without adequate pharmaceutical care: A randomized controlled study. Clin Epidemiol Glob Health. 2023;20(20):101208 [CrossRef] | [Google Scholar]